ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Health Economics, Medical School, National and Kapodistrian University of Athens, Athens, Greece.
2Department of Healthcare Management, University of West Attica, Athens, Greece.
Department of Health Economics, Medical School, National and Kapodistrian University of Athens, 75, M. Assias Street, 11527, Athens, Greece.
Email: karafedis@yahoo.gr
Received : December 21, 2023,
Accepted : January 04, 2024
Published : January 11, 2024,
Archived : www.jclinmedcasereports.com
Introduction: Violence in the work environment of healthcare providers has increased dramatically in the last decade internationally. By insanely violating the personal rights of health professionals, there are attacks on healthcare providers, both from abroad and from the domestic environment, attacks that ultimately have adverse health effects and the performance of healthcare professionals. These effects clearly affect healthcare providers, as it is common for professionals working in an environment of fear and resentment to be unable to perform at their best, to provide inadequate or poor quality care, ultimately affecting patient safety.
Purpose: The main interest of this article is to identify the main causes that cause the occurrence and development of the phenomenon of violence in the Workplaces of the Health Sector, through the review of articles and modern empirical studies.
Methodology: Searches of articles and research studies were carried out in the electronic databases “Pubmed” and “Cinahl” and in the Association of Greek Academic Libraries (HEAL-Link), with main criteria for identifying the forms of violence that develop most and the factors that cause them in the last two decades.
Results: The development of violence that affects health professionals causes a variety of symptoms that seriously affect the health and personality of the individual. The harassment that comes from either a colleague, senior in the hierarchy, patients or third parties, leads to serious psychosomatic illnesses but at the same time shakes the social position, career path and financial situation of the health professional. Conclusions: The present review highlighted a number of published studies documenting the extent of the problem. Violence in the work environment of healthcare providers is a real, serious global problem for healthcare professionals and must be addressed both in terms of prevention and early intervention.
Keywords: Workplace violence, Health professionals, Healthcare organizations, Aggression.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Karaferis Dimitrios 2024
Workplace violence has become an alarming phenomenon around the world and is increasing [1]. The true magnitude of the problem is little known, but recent information suggests that the current knowledge is just the tip of the iceberg [2]. More and more cases of violence that seemed unexpected years ago in hospitals, endangering the life, honor and integrity of medical professionals such as doctors, nursing staff and the rest of the staff working in these areas, have been "targeted" (especially in emergencies during speech time) and other medical institutions (psychiatric hospitals and health centers) [3]. Increasingly, workers are expressing growing concerns about violence perpetrated by patients and visitors, with many reporting that they rarely or never feel safe in the workplace. Compared to workers in other sectors, it is thought that health workers have four times the exposure rate to workplace violence [4, 5]. The main concern of every health system is to promote health while ensuring equality of opportunity [6]. The medical staff provides a special type of service. From his work, he treats wounds and diseases, determines the causes of diseases, supports the well-being and health of the world's population. They often treat people who are unable to take care of themselves, who are in desperate need of attention and care due to illness, age or other conditions. Both health workers and patients need a calm and stable environment in which they feel supported and safe [7]. For health workers, violence is a complex and dangerous occupational hazard [8]. If health professionals feel that they are at risk in terms of the population they serve, they can subconsciously develop a defense mechanism that can lead to the formation of impersonal relationships with patients and negatively affect the quality of care they provide. This means that people at risk of violence may be treated with less trust, less commitment, and even complete disregard [9, 11]. In Greece, the Panhellenic Medical Association, based on International Research, points out that at least 25% of doctors working in emergency departments faced physical or verbal violence in 2018-2019 and wants to highlight the huge dimensions that the phenomenon of violence is currently taking on. This article aims to present the forms of violence, mainly the main factors in the presence and continuous increase of violence in health care providers [12].
Definition of workplace violence: The term Workplace Violence (WPV) refers to attacking an individual and threatening his or her safety and integrity. More generally, it is directed at insults, threats, physical or psychological attacks made by people who endanger the health, safety or well-being of employees inside or outside the institution. It can include a racial or sexual aspect, occurs in almost any workplace and ranges from threats to murder. According to the World Health Organization (WHO), workplace violence is "deliberately enforced in the form of threats to other people or groups who are physically or in working conditions, which leads to an increased likelihood of injury, death, psychological harm, underdevelopment or deprivation" [13]. The National Organization for Occupational Safety and Health (NIOSH) defines workplace violence as: "Violent behavior, such as physical assault or threats of assault against people at work or on duty" [14,15]. The European Commission considers workplace violence "when an employee is attacked in cases directly related to his work, it defines it as any situation in which he has been threatened or assaulted, and in which these conditions directly or indirectly endanger his safety or involve an explicit or implicit challenge to his health" [16]. The terms "violence" and "aggression" are not easily distinguishable from each other. For this reason, it is considered as a synonym in our study [17].
Forms of violence and types of relationships in which violence develops: The violence in his statement takes many forms, covering all acts and threats of physical violence against employees, from intimidation and intimidating behaviors, harassment and verbal harassment to physical attacks at the workplace [18]. However, the symptoms of violence can be classified in the following four cases [19]:
a) Physical violence, caused by penetration, pushing, shoving, coercion or assault into a worker's "immediate" personal space for the purposes of coercion, exploitation and benefit; between 8% and 38% of health workers are subjected to physical violence at some point in their career.
b) Verbal violence, is verbal harassment or abuse (loud protests, collective noises, innuendo, sarcastic or manipulative comments, sarcasm, sarcasm, elitist attitudes, threats or insults) and can be expanded by derogatory racist or sexual comments. It manifests itself due to a lack of respect and appreciation for other people's people with the main goal of reducing the personality of others. Verbal abuse in general seems to discourage staff, as they experience it as a blow to their self-confidence and professional credibility, and may perceive it as a response to their efforts, i.e. they are attacked while trying to cope. instead of making sure it looks like you're living a traumatic life. They feel like they are being attacked and they are going through this. Verbal abuse is as harmful as physical violence, and the resulting consequences are thought to be: 1) physical (headache, back pain, fatigue 2) emotional (depression, post-traumatic stress syndrome), and 3) behavioral (refusal to work, aggression, increased smoking) [20].
c) Sexual violence, refers to an attempt to forcibly engage in sexual activity without a person's consent.
d) Psychological or emotional violence, is an act of "trauma" to the victim, which may constitute a threat of pressure acts or tactics to dominate or humiliate the victim.
Another decoupling between violence, which is more closely related to the internal environment of the organism in health, is [21, 22].
• Lateral violence, which is refers to deceptive behaviors that occur between individuals at the same level of the organization's health hierarchy, i.e. nurses.
• Vertical violence, which is refers to the violence that occurs between individuals at different levels within the health hierarchy of an organization. We can distinguish the development of two directions.
a) from top to bottom, in this case we refer to events that interpret the abuse of legitimate power within the organization.
b) from the bottom up, in this case we refer to any incident is connected with unofficial force.
In addition to the previous forms of violence, we can also distinguish the types of relationships in which violence develops in the working environment of health care providers. In particular, we recognize three main types of violence [23].
a) patient or visitor with staff: we refer to the development of a type of violence, where the patient himself, his escorts or all together attack the staff of the health service provider. Based on the literature it is shown as the most common source of violence [17].
b) staff-to-staff: these are incidents that develop between colleagues or between subordinates with supervisors or management.
c) third parties with staff: includes all those who come to health service providers without having as their main purpose to be examined or hospitalized, such cases are.
1) suppliers who are dissatisfied.
2) homeless, alcoholics, drug addicts, mentally disturbed people who resort to health care providers without being fully conscious or in despair.
3) people arriving for the purpose of robbery, as health service providers have insufficient security.
4) personal relationships of employees who are not related to health service providers, i.e. spouse or relatives of those who come to vilify the employee in his work environment for the resolution of disputes between them or third parties who come to resolve financial disputes or other reasons.
The introduction of violence into the work environment of health care organizations: Work plays an important role in a society where employment is underestimated. He confirmed that the study has many health benefits. However, when the workplace becomes a "toxic environment", problems arise in which workers may become victims or perpetrators in the workplace [24]. Violence always increases in times of crisis and poverty, which is why poor countries like India have serious problems with violence in hospitals. However, this phenomenon has now passed in the Western world and has highlighted the need for competent organizations such as the World Health Organization and the World Medical Association to take steps to stop it. The healthcare sector in European Union countries has now been included in a dangerous service environment and, as evidenced by numerous studies, has been identified as one of the sectors where violence has the biggest problem, especially with health professionals (doctors, nursing staff and other health workers) who are considered to be at risk of violence. The areas where most cases of violence occur are: emergency departments, intensive care units, operating rooms, nursing rooms, laboratories and administrative services that serve the public directly. There are also acute violence problems in mental health facilities and services, where attacks continue [25].
Studies related to the development of violence in Healthcare Providers: A large number of published studies conducted in different countries document the scope of global problems over the past twenty years. In the United States, the healthcare sector is one of the top sectors in terms of non-fatal workplace assaults in 2000, 1% of non-fatal injuries caused by violence against workers were in the health sector [26]. According to current studies and reports on workplace violence in the health sector, about 25% of workplace violence incidents occur in the health sector, and more than 50% of health workers experience violence at work. According to a study conducted by the American College of Emergency Physicians in 2018, 47% of more than 3,500 doctors have been attacked, and the attacker has been a patient or a staff member [27-29]. In a study developed from 2001 to 2002 in the United Kingdom, the National Health Service (NHS) reported 95,501 cases of violence and assault against its employees. Verbal harassment is the most common form of violence in the workplace, and nurses are increasingly being targeted. Weapons are often carried in the emergency department, and many working days are lost due to injuries caused by physical attacks [30]. It has also been reported that there is a high incidence of workplace violence among nurses in South Korea. A recent study reported that 71% of nurses had experienced at least 1 aggressive violence in the past year. Verbal harassment (63.8%) had the highest increase and bullying was the lowest presentation (9.7%) [31]. A survey conducted in China in 2008 found that 80% of healthcare professionals agree that the doctor-patient relationship is bad or very bad. a survey conducted by the Chinese Medical Association (CMDA) in 2014 showed that 60% of doctors surveyed had experienced verbal abuse from patients and relatives, and 85% of professionals who physically assaulted 13% of doctors had experienced workplace violence. The latest survey of Chinese medical professionals [32]. In Japan, in a survey developed among 8,771 respondents, 36.4% of respondents said that they had experienced workplace violence from patients or relatives in the past year, 15.9% of them experienced physical assault, 29.8% verbal harassment and 9.9% sexual harassment [33]. A recent survey of 265 health workers found that 44.7% of respondents said they had experienced violence in the past year. According to the type of violence, verbal harassment was reported at a rate of 62.3%, physical violence at a rate of 60.4% and sexual harassment at a rate of 2.6% [34].
The Indian Medical Association (ΙΜΑ) reports that 75% of doctors have experienced verbal or physical abuse in hospitals, and violence is the most common cause of anxiety for 43% of doctors [35]. The most violence was reported at the emergency care points and 70% of the violence cases were initiated by the patient's relatives. The incidence of reported violent crimes against doctors in India has been increasing significantly from 2006 to 2017 [36]. A survey conducted in 2009 with 1,091 workers in Saudi Arabia [37] found that about 28% had been subjected to at least one violent incident in the previous year. while 92.1% developed at the emotional level, 7.9% developed at the physical level [38]. In a more recent study, 48.6% of the participants reported that they had been exposed to violence at least once in the past year [39]. According to a survey conducted in Israel, at least 56% of doctors have been subjected to verbal abuse and 16% to physical violence during their careers. Doctors, psychiatrists and nurses working in emergency departments were found to be the most exposed risk group to violence [40]. In a survey conducted with emergency, intensive care and psychiatric nurses in Turkey, it was found that most of the nurses (60.8%) were subjected to verbal or physical violence by patients, visitors or health workers [41, 42].
A study developed in Swiss hospitals showed that 95% of nurses have experienced violence during their careers, 72% suffered verbal abuse and 42% physical violence in the past 12 months [43].In a Spanish survey of almost 8,000 health workers, 11% reported having experienced physical assault and 64% had experienced threatening behavior, bullying and insults in the previous year [44]. In a survey of 915 health workers in Italy, 59.1% said they had experienced violence and 65.9% said they had seen violent incidents occur, 40.2% were subjected to verbal abuse and 11.5% to physical violence. Among health professionals, 53.4% reported anxiety at work and felt that it was related to patients and visitors [45].In Greece, a systematic study conducted at the General University of Patras, the results showed that violence against health workers is very common, the level of violence development reported in the medical environment was high last year with 87.5% and 62.9% [30]. In Portugal (which has almost the same working culture as Greece), 36.8% of hospital medical staff reported violent incidents last year. Despite the special importance of understanding health violence, most studies on violence in health systems have been limited to measuring its scope and have mostly focused on emergency departments and psychiatric departments [46, 47]. Other studies have focused on violence between decembers of staff and violence by staff towards patients [48-53].
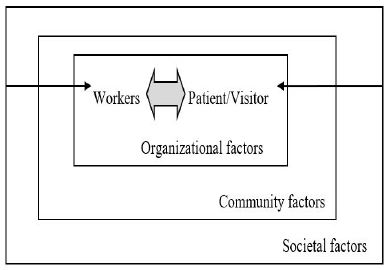
Factors that reveal and exacerbate the phenomenon of violence in health care providers: The presentation and Deceleration factors of the phenomenon of violence are based on the development of the relationship between health workers and patients or visitors [54]. In general, the experience of illness and the procedures that must be followed by health care providers cause fear and anxiety. Patients and visitors are dependent on medical staff, and this relationship has a key role in the care process. The interactions of the developing relationship between health care workers and patients or visitors may increase the likelihood of violence. Factors that may weigh on this relationship include poor, inappropriate, inadequate or incorrect communication, misunderstandings, brief comments on how information is shared between professionals and patients, unfulfilled or unrealistic expectations on behalf of patients and their families, dissatisfaction with the treatment process and / or disagreement with the doctor. The relationship may be affected by the lack of communication, misunderstandings, brief comments on how information is shared between professionals and patients, unfulfilled or unrealistic expectations on behalf of patients and their families, lack of trust between professionals and patients, poor patient compliance [55, 56]. As can be seen in the figure below, Patients and Visitors enter the care system, it is an unfamiliar environment, they are concerned about the development of the procedure, they always take the utmost care of their health and expect to leave as soon as possible. On the other hand, health professionals (workers) must welcome and accompany patients and visitors, guide them so that the prescribed rules and procedures are followed. It is necessary to establish relationships that are especially important for the development of the patient's health. When the relationship between the patient and the healthcare provider passes decently, the patient's expectations are verified, he feels safe and secure, he is healthy according to the instructions given to him. Conversely, if the patient's expectations are not confirmed, the relationship between the patient and the medical professional decays and he becomes uncomfortable with the procedure, which can push him to attack.
Three main groups of factors affecting the relationship between health workers and patient visitors and leading to the development of violent incidents have been found: a) organizational factors, b) community factors, c) societal factors. Schematically deciphering this relationship as below [57, 58]: Organizational factors can play an important role. Most workplace conflicts arise from organizational, policy and business structures. Staff shortages, worker job segregation, management, communication, workload and the pressure experienced by workers are key factors that can increase the risk of violence due to longer patient waiting times and the fact that health workers often work alone with patients. Factors that create workplace stress, such as ineffective communication, lack of resources, low support and monitoring, excessive workload, poor workgroup relationships, mismatched values, and imminent changes in the workplace, such as downsizing or restructuring of an organization, can increase the risk of workplace attacks. Moreover, inadequate lighting, inadequate security of facilities and the ability to access objects that can be used as weapons may increase the risk of violence [59-62]. In any case, health institutions (hospitals, health centers, local dispensaries, etc.), if they are embedded in the communities in which they operate, these communities may influence the type or level of violence experienced by the workplace. High levels of violent crime, drug use, gangs in a community, low levels of community funding sources, distrust or decommunization between residents and minorities, and community factors such as auctions can contribute to the occurrence of violence in health services. The evidence linking higher levels of violence with troubled populations is consistent. People who live in deprived areas or have problems (such as those with mental illness or learning disabilities living domestically) may pose a greater risk of violence to medical staff. In a recent survey of general practitioners in the UK, doctors serving disadvantaged populations reported higher levels of verbal harassment and a greater risk of serious incidents than doctors working in other fields. The fear of working with such client communities can affect the quantity and quality of health services available in deprived areas [63-71].Social factors such as social inequality overshadowed by the risk of workplace violence, gender discrimination, changes in social norms related to the acceptance or reduction of aggression play a particularly important role. Social views play a special role in ethical issues, for example in abortion clinics in parts of the United States where health care providers are subjected to violence by anti-abortion campaigners. Finally, health care providers can provide care in dangerous environments, such as areas severely damaged by war or war refugees, and by their very nature workers are exposed to increased physical and mental risks [72,73].In Greece, the intensification of the discussed phenomenon of violence may be directly related to the growing unrest in an ever-changing society strongly affected by the economic crisis. Violence is an interactive phenomenon in the sense that representatives of different classes participate in what they interact with.
The main factors for the occurrence and aggravation of violence in the medical field are the following:
• Stress [74].
• Intense concern about the patient himself or the consequences of the accompanying health condition [75].
• Complete lack or poor state of existing infrastructure and resources in health care providers
• Long waiting times and services for citizens.
• Inadequate and inadequate management of health sector personnel in both large urban and rural structures.
• Crowding out some health professionals and avoiding others for their reputation [76].
• Poor maintenance conditions, high temperatures, high humidity, extreme cold, poor lighting and air quality, high noise levels and overcrowding have been reported to be associated with increased levels of human aggression [77].
• An increase in people under the influence of alcohol and drugs.
• An increase in people with mental disorders.
• 24-hour / 7-day operation, especially in the hospital.
• Inadequate security measures.
• Necessary close contact between health workers and patients.
• Do not work alone.
• Working hours in health institutions (night and rolling).
• nLow harmonization of working groups and support for supervision [68].
• Increased hospital Workload as a result of major shortcomings in Primary Care Development.
• Insufficient funding and insufficient personnel .
• Reducing wages, freezing wages and using part-time jobs [78].
• Misinterpretation or misinterpretation of personnel behavior in health.
• Deliberate indifference of medical personnel and exploitation of patients.
• Lack of policies aimed at preventing violence in the health sector.
• Insufficient training of personnel for the correct response in the event of a case of violence reporting incidents of violence, the victim was condemned by the attackers or the escort or was born out of fear of exposure, guilt, shame or revenge and sometimes lack of time and unwillingness to fill in documents with information that any action, part of the organization-level work in which the attack was carried out or, concerns about the consequences, feelings of faith [79,80] .
• Insufficient development of laws and penalties for those who commit violence in the health sector.
The study showed the role and magnitude of the phenomenon of workplace violence in healthcare providers. The last twenty years have been characterized by a dramatic increase in the international arena. This is a multidimensional and complex phenomenon that often seriously affects the health and personality of health professionals, resulting in lower job satisfaction and organizational commitment, and negatively affecting the quality of care provided. Due to the high level of underreporting of violent incidents by medical professionals, appropriate measures should be taken to prevent and combat this phenomenon, develop relevant preventive and therapeutic studies, as well as change the legal framework, frame of reference and structure on which the specialist is based. declare the violence received in their work.
Declaration of Interest: The authors declare no conflict of interest.
Conflict of Interest: Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
Author’s contribution: All authors were involved in all steps for preparation of this article, including final proofreading and gave final approval of the version to be published.
