ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1ENT Department, Unidade Local de Saúde Entre o Douro e Vouga, Portugal.
2ENT Department, Instituto Português de Oncologia de Lisboa - Francisco Gentil, Portugal.
3Reconstutive and Plastic Surgery Department, Instituto Portugês de Oncologia de Lisboa - Francisco Gentil, Portugal.
4ENT Department, Unidade Local de Saúde Lisboa Ocidental, Portugal.
5Unit for Multidisciplinary Research in Biomedicine, Institute of Biomedical Sciences Abel Salazar, University of Porto, Porto, Portugal.
ENT Department, Unidade Local de Saúde Entre o Douro e Vouga, Portugal.
Tel: +351-917095050; ORCID: https://orcid.org/0000-0002-8930-9383; Email: veracms@hotmail.com
Received : Aug 28, 2024,
Accepted : Sep 18, 2024
Published : Sep 25, 2024,
Archived : www.jclinmedcasereports.com
Background: Ewing Sarcoma, is a highly aggressive malignancy, extremally rare in the nasal and paranasal sinuses. The treatment landscape for Sinonasal Ewing Sarcoma (SNES), is predicated on a multimodal approach encompassing surgery, chemotherapy, and radiotherapy. Recurrence in SNES, although rare, significantly complicates management and adversely impacts prognosis.
Case report: A 30-year-old female, previously treated for SNES, exhibited recurrence after 15 years of remission, presenting with superior palpebral edema and no other symptoms. Diagnostic investigations confirmed the recurrence, with imaging showing a lesion on the left nasal bone. A multidisciplinary approach led to surgical resection, achieving disease-free margins and an aesthetic reconstruction with titanium mesh and a frontal flap, and adjuvant radiotherapy and chemotherapy.
Conclusion: Recurrent SNES represents a significant challenge in oncology. The management of recurrent disease is customized for each patient, weighing the disease’s severity against the potential effects of therapy on life quality.
Keywords: Ewing’s sarcoma; Nose neoplasms; Neoplasm recurrence; Local; Reconstructive surgery.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Miranda V (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Ewing Sarcoma, is a highly aggressive malignancy primarily affecting bone and soft tissue among children and young adults [1]. Although this malignancy commonly involves the long bones and pelvis, Sinonasal Ewing Sarcoma (SNES) represents a rare and unique subset, manifesting within the nasal and paranasal tract. The incidence of SNES is exceedingly low, contributing to less than 1% of all cases, thereby complicating both the diagnostic process and therapeutic approaches due to limited clinical experience and scarcity of literature [2,3].
Ewing Sarcoma is characterized by the pathognomonic chromosomal translocation t(11;22)(q24;q12), resulting in the EWSR1-FLI1 fusion gene, which act as aberrant transcription factors driving oncogenesis [1]. This molecular signature not only serves as a diagnostic biomarker but also offers potential targets for therapeutic intervention, highlighting the importance of molecular diagnostics in the management of SNES [4].
Clinically, SNES presents a diagnostic challenge due to its nonspecific symptoms, such as nasal obstruction, epistaxis, and facial swelling, which are commonly attributed to more prevalent nasal conditions. This often results in diagnostic delays and highlights the necessity for clinical vigilance and consideration of SNES in the differential diagnosis of persistent nasal symptoms unresponsive to standard treatments [5]. Advanced imaging modalities, including MRI and CT scans, play a main role in delineating the tumor’s extent and planning surgical intervention, while histopathological and molecular analyses confirm the diagnosis [6].
The treatment landscape for SNES, mirroring that of Ewing Sarcoma elsewhere, is predicated on a multimodal approach encompassing surgery, chemotherapy, and radiotherapy. The overarching goal is to achieve local control and address systemic disease, with chemotherapy regimens such as VIDE (Vincristine, ifosfamide, doxorubicin, and etoposide) serving as the backbone of treatment. Surgical resection, when feasible, aims for complete tumor removal while preserving vital structures and function, underscoring the need for individualized treatment planning and multidisciplinary care [7].
Despite advances in understanding and managing Ewing Sarcoma, the prognosis for SNES remains unclear, with outcomes closely tied to factors such as tumor size, extent of local disease, and response to therapy. The rarity of SNES limits large-scale epidemiological and clinical studies, necessitating reliance on case reports and institutional experiences to guide treatment and prognosis strategies [8].
Recurrence in SNES, although rare, significantly complicates management and adversely impacts prognosis. It demands a comprehensive re-evaluation and an individualized therapeutic approach, often involving a combination of surgery, chemotherapy, and radiation, tailored to the specific recurrence pattern and previous treatments received [3,5,6]. The prognosis for recurrent SNES remains uncertain, with outcomes heavily influenced by the recurrence’s extent and the feasibility of achieving complete surgical resection [8]. Advances in molecular biology have begun to unveil potential targets for therapy, offering hope for more effective treatments in recurrent settings [4].
Objective
The objective of our study is to describe a case of recurrent Sinonasal Ewing sarcoma, following a 15-year follow-up period, which was treated with surgical intervention. The surgical approach involved the excision of the lesion and the reconstruction of a pedicled frontal flap to optimize the aesthetic outcome.
We report the case of 30-years-old female patient, who was treated in adolescence for Sinonasal Ewing Sarcoma involving the left nasal cavity and ethmoid sinus. Treatment consisted of chemotherapy, following the VIDE protocol, and endoscopic sinonasal surgery (total left ethmoidectomy). Throughout an extensive follow-up period, there were no clinical or radiological indications of recurrent disease.
After 15 years of follow-up, the patient presented to our Otolaryngology Department with a recent and persistent onset of superior palpebral edema. There was no complains of nasal obstruction, epistaxis, headaches, proptosis, diplopia and the eye movements were normal. The patient had no comorbidities or history of tobacco use. Flexible nasal endoscopy revealed signs of previous surgery with ethmoidal cavity without mucosal edema or identifiable masses. A discrete mass was palpable in the left nasal bone adjacent to medial canthus. A fine needle cytology from medial canthus was performed and sent for cytological analysis. Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) were scheduled. She underwent an ophthalmologic examination, which revealed a normal visual acuity (20/20) and had no impairment on ocular alignment or ocular movements and a normal ocular fundoscopy.
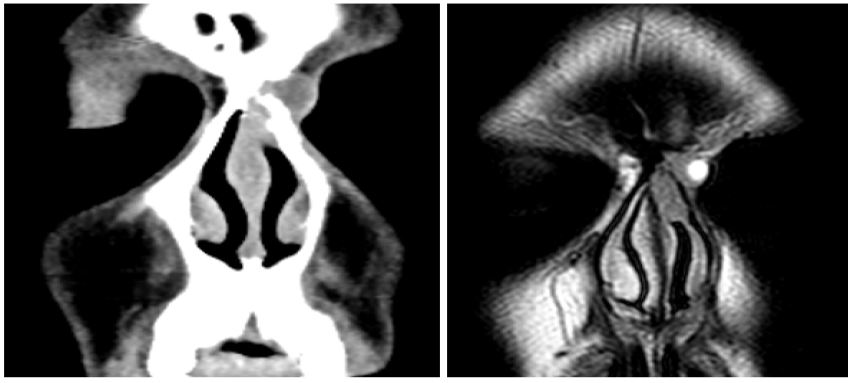
CT and MRI showed a lesion on the left side of the nasal pyramid (18 x 16 x 13 mm, longitudinal, anteroposterior, and transverse axes, respectively) invaded the left nasal bone and the area of the frontonasal suture (Figures 1 and 2). It abuts, without invading, the anterior portion of the ipsilateral orbit’s inner wall. That lesion was suspicious for a recurrence of Ewing’s sarcoma. The pathological evaluation with hematoxylin-eosin staining revealed a neoplasm composed of small, round, blue cells with PAS-positive cytoplasmic granules. Immunohistochemistry demonstrated positive staining for CD99 antigen and vimentin, with negative staining for cytokeratin AE1/AE3. The FISH analysis revealed rearrangement of the EWSR1 gene in 100% of the evaluated nuclei. These findings support the diagnosis of recurrent Ewing’s sarcoma. Positron Emission Tomography (PET) was then performed for staging and treatment planning, and no metastatic lesions were detected.
Therapeutic intervention
The patient’s case was presented to our institution’s multidisciplinary tumor board, which recommended surgical resection followed by another round of chemotherapy and possible radiation therapy, pending surgical margins and final pathology.
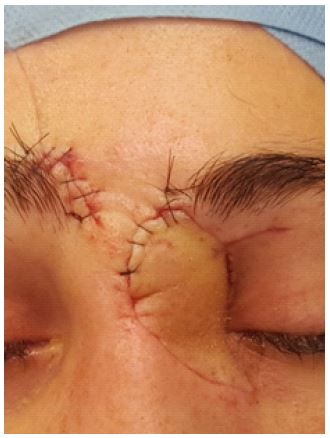
The surgery was planned with a consultation with a plastic surgeon, aiming to achieve complete disease resection and minimize the aesthetic impact. Through a prolonged Lynch incision extending to the glabella region, the lesion was resected en bloc, encompassing the glabellar and nasal bones, lamina papiracea, and adjacent skin (Figure 3). Negative margins were achieved through frozen section analysis. The osseous defect was corrected by placing an adjustable titanium mesh (Figure 4). The cutaneous defect was corrected by performing a contralateral frontal flap (Figure 5). The frontal flap underwent a second-stage procedure for functional optimization three weeks later (Figure 6), resulting in a satisfactory aesthetic outcome.
Follow-up and outcomes
Postoperative histopathologic examination revealed confirmed the Ewing sarcoma diagnosis, with positive osseous margin. Adjuvant radiotherapy (Intensity-Modulated Radiation Therapy – IMRT) with a total of 45 Gy and chemotherapy with ifosfamide was performed. Twelve-month postoperative follow-up showed no evidence of tumor recurrence.



This case of recurrent Sinonasal Ewing Sarcoma in a 30-year-old female, initially treated with the VIDE protocol and endoscopic surgery, and presenting 15 years post-treatment without recurrence until now, provides a unique contribution to the literature on long-term outcomes and management of SNES. The atypical presentation, characterized by superior palpebral edema emphasizes the necessity for vigilance in follow-up protocols, even many years post-treatment [9].
Recurrent SNES represents a significant challenge in oncology, necessitating a multidisciplinary approach to optimize treatment outcomes. The management of recurrent SNES is tailored to the individual patient, balancing the aggressiveness of the disease with the potential impact of treatment on quality of life. This case highlights the rarity of late recurrences in Ewing sarcoma, underscoring the importance of long-term vigilance even beyond the first decade post-treatment. Furthermore, it illustrates the effectiveness of combining oncologic resection with reconstructive techniques to achieve both curative and cosmetic objectives, presenting a significant contribution to the limited literature on long-term management strategies for recurrent SNES.
Funding: No funding sources.
Conflict of interest: None declared.
Ethical approval: Not required.
