ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*11Postgraduate Scholar, Department of Shalya Tantra, Mahatma Gandhi Ayurved College, Hospital and Research Centre, Salod (Hirapur), Datta Meghe Institute of Medical Sciences (Deemed to be University), Wardha, Maharashtra, 442001, India.
2Associate Professor, Department of Shalya Tantra, Mahatma Gandhi Ayurved College & Hospital and Research Centre, Datta Meghe Institute of Medical Sciences (Deemed To Be University) Salod (H), Wardha Maharashtra, India.
1Postgraduate Scholar, Department of Shalya Tantra, Mahatma Gandhi Ayurved College, Hospital and Research Centre, Salod (Hirapur), Datta Meghe Institute of Medical Sciences (Deemed to be University), Wardha, Maharashtra, 442001, India.
Email: Tel: +918329573966;
Email: drabhishekmavale@gmail.com
Received : Oct 04, 2024,
Accepted : Nov 06, 2024
Published : Nov 13, 2024,
Archived : www.jclinmedcasereports.com
Symmetric with the posterior portion of the vaginal opening, the Bartholin’s glands are crucial to the female reproductive system. These two tiny glands are responsible for vaginal lubrication and mucus discharge. Mucus accumulation in gland ducts leads to the frequent development of cysts in the glands. These cysts should be closely watched as they can develop into carcinomas. Larger abscesses and cysts are located in the lower vestibular area; they usually cause edema and erythema. A biopsy is a useful tool for differentiating between differential diagnosis and Bartholin’s gland cysts. Larger cysts need to be treated by a doctor, although smaller cysts might not hurt and can be ignored. There are several possibilities for therapy, including as CO2 laser. Healing and recovery depend on the severity of infection and course of treatment. Cysts in the Bartholin gland represent 2% of gynaecologic visits annually. The management of Bartholin gland cysts has changed throughout time, going from a difficult, bloody operation needing general. Treatments for Bartholin gland cysts may appear straightforward at first, but they might become more difficult if the cysts recur or if it becomes difficult to distinguish between benign cysts and malignant tumours. The history of treating Bartholin gland cysts is examined in this article, along with the application of conventional methods such as excision, fistulisation, marsupialization, and carbon dioxide laser and silver nitrate cauterization. Current modifications are covered, such as the excision method of local application of panchawalkal ointment in devising treatment for recurrent cysts.
Keywords: Bartholin’s glands; Cysts; Abscesses; Vulval lubrication; Female reproductive system.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mavale A (2024).
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
An important component of the female reproductive system are the Bartholin’s glands. Danish anatomist Casper Bartholin was the first to characterize the glands in the 17th century. The organs’ main job is to produce mucus to provide vaginal and vulval lubrication. Infections and abscess development are common in the Bartholin’s glands, which can cause vestibular discomfort and dyspareunia. Although various issues may result in Bartholin’s cyst, abscess, or cancer, bacterial cultures are linked to the origin of these diseases [1]. Research has shown that Bartholin’s carcinoma can be diagnosed in people with uncommon blood types, suggesting a possible relationship between the blood type antigen and Bartholin’s gland tumour. The research on Bartholin’s anatomy, physiology, and pathology will be reviewed in this article, along with treatment options for illnesses of the Bartholin’s glands [2].
The two pea-sized glands known as the Bartholin’s glands, or larger vestibular glands, are situated at the back of the vaginal opening. The oval-shaped glands are situated lateral to the bulbocavernosus muscle, with an average size of 0.5 cm. The glands bear similarities to Cowper’s or bulbourethral glands seen in males [3]. The glands are attached to ducts that lie between the hymenal border and the labia minora, and they are about 2.5 cm wide. The glands release mucus into the vaginal vestibule through these channels. On either side of the vaginal opening, the ducts open at four and eight o’clock in the vaginal vestibule. Embryologically, the Bartholin’s glands arise from the urogenital sinus and consequently, utilize the external pudendal artery as a blood source. The gland is innervated by the pudendal nerve. The lymphatic drainage of Bartholin’s glands includes superficial inguinal and pelvic nodes [4].
Lesions in the Bartholin’s gland can occur in the form of carcinomas, a rare type of gynecological tumours that accounts for 2-7% of vulvar carcinomas. This type of vulvar growth is carefully monitored among postmenopausal women who are more prone to Bartholin’s malignancy [5]. The median age at which Bartholin’s gland cancer is diagnosed is 57 years old and carcinoma incidence is highest among women in their 60’s. The 2 common types, adenocarcinoma and squamous cell carcinoma, account for 80-90% of primary cases. The remaining 10-20% of cases include transitional, adenoid-cystic or undifferentiated carcinomas. Human papillomavirus is only related to squamous cell lesions. Benign tumors are rarer than carcinomas [6].
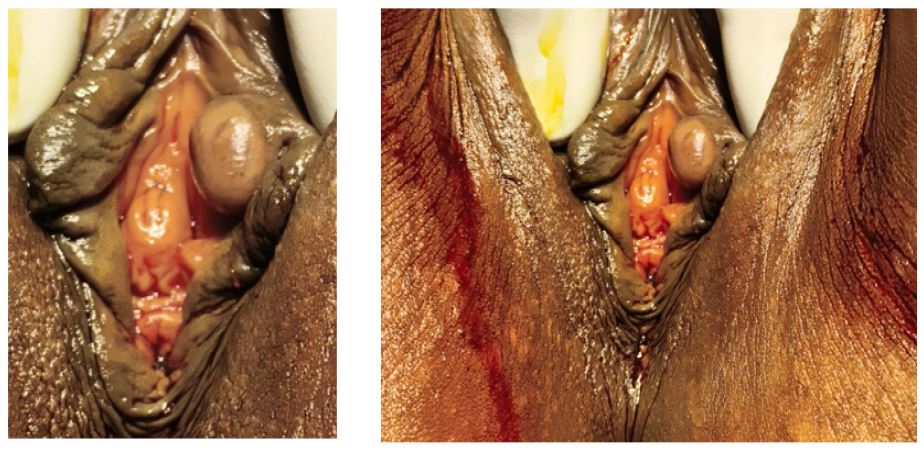
A 23-year-old female patient arrived at the Shaya Tantra Department of MGACH & RC Salod, Wardha, complaining of discomfort and irritation before and after micturition, as well as a sense of mass in the vaginal area that was swelling daily. She also attended the Shalya Tantra OP Department for additional care. An instance of K/C/O-hypertension and diabetes mellitus from an ancient medical record No asthma or K/C/O tuberculosis. A recent RBS Post meal: 132 mg/dl and Fasting: 110 mg/dl. HbA1c=5.6% The ECG shows a normal sinus rhythm. During a physical assessment the tumour must largely be found in the Left fold of labia, the surrounding skin must not be injured, and there must be at least a modest amount of glandular epithelium present, as illustrated in (Figure 1). A well-defined, transversely moveable pedunculated mass, measuring about 0.5×0.5 cm, was seen in the tumour.
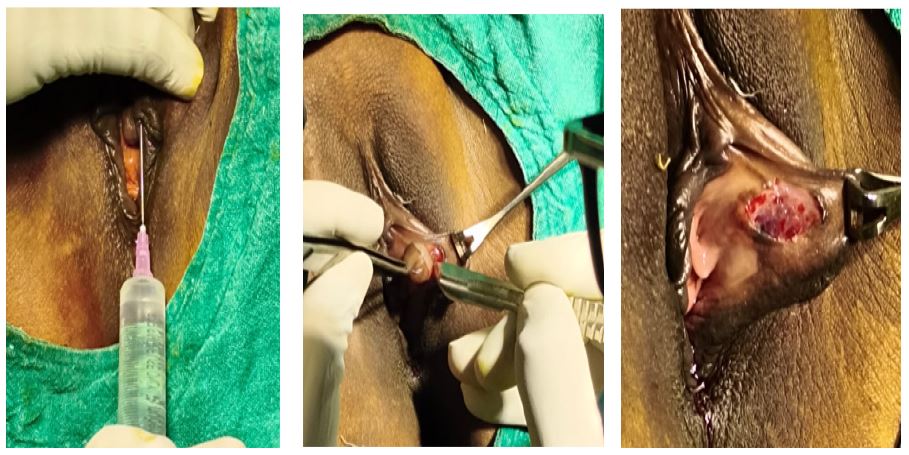
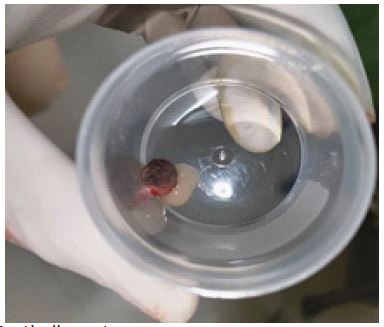
Local anesthetic was used for the surgical operation. The mass’s pedicle was sliced in a straight line, and the dissection was then deepened to the subcutaneous plane. After carefully removing the tissue containing the bartholine cysts and achieving hemostasis, the main incision was closed with Vicryl 2-0. As seen in (Figures 2 and 3), the patient had a smooth postoperative course and a good level of tolerance for the surgery. He was released with an appointment for routine follow-up care.
Numerous lesions in the labia and vagina might mimic disorders of the Bartholin glands. When such circumstances arise, a differential diagnosis for the tumour or abscess should be taken into account. Differential diagnosis includes endometriosis, syringoma, accessory breast tissue, folliculitis, urethral diverticula, hidradenitis suppurativa, chancroid, gonorrhoea, syphilis, vaginitis, warts or Bartholin’s gland cyst, leiomyomas, fibroma, hernia, hidradenoma, hematomas, lipomas, endometriosis, syringoma, and accessory breast tissue [7].

Informed consent: Patient’s consent was obtained for collecting information and producing images with maintenance of privacy and confidentiality for use in research/academic purposes.
