ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Department of Emergency and Critical Care Medicine, Nara Medical University, 840 Shijo-Cho, Kashihara City, Nara, Japan.
Department of Emergency and Critical Care Medicine, Nara Medical University, 840 Shijo-Cho, Kashihara City, Nara, Japan.
Tel: +81-744-22-3051 & +81-744-22-4121;
Email: k190143@naramed-u.ac.jp
Received : Oct 11, 2024,
Accepted : Nov 12, 2024
Published : Nov 19, 2024,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Osaki T (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
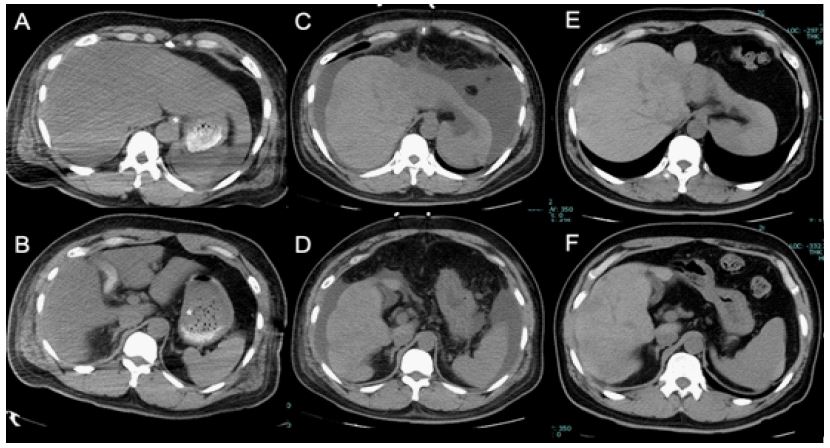
A 46-year-old man with a history of mood disorder self-injured his left radial artery using a kitchen knife. Upon hospital arrival, his blood pressure was 61/36 mmHg, and he soon deteriorated into cardiac arrest. After 8 min of resuscitation, he regained spontaneous circulation and was admitted to the intensive care unit. An Abdominal Computed Tomography (CT) on admission revealed mild steatosis in the liver (Figures 1A and B). Laboratory tests on admission revealed mild elevation of serum Aspartate Aminotransferase (AST)/ Alanine Aminotransferase (ALT) levels (113/78 IU/L) with an International Normalized Ratio (INR) of 1.28 and a total bilirubin level of 0.3 mg/dl. These values increased to 3,662/3,041 IU/L and 2.37, respectively, after 8 h. However, the total bilirubin remained at 0.5 mg/dl. On day 4, serum AST/ALT levels increased to 7,397/2,542 IU/L. Although serum AST/ALT levels began to decrease thereafter; the total bilirubin level increased to 12.6 mg/dL by day 15. A follow-up abdominal CT on day 20 revealed liver atrophy with ascites (Figures 1C,D). Mild atrophy persisted until day 33 (Figures 1E,F). Laboratory test results returned to normal by day 105. The patient survived hospitalization without any complications.
Ischemic hepatitis can result from severe circulatory failure and is characterized by transient, rapid, and massive increases in serum aminotransferase levels [1]. The in-hospital mortality rate can reach up to 60% [2]. Typically, diagnostic imaging is not required, and hepatic atrophy is rarely assessed using CT. Generally, ischemic hepatitis occurs within 0 to 5 days, while drug-induced liver injury often occurs after 7 days [3]. In this case, serum AST/ALT levels increased to four digits within 8 h of admission. The clinical course of this case was consistent with ischemic hepatitis rather than drug-induced liver injury.
Acknowledgments: None.
Conflicts of interest: None.
Ethical statement: Informed consent for publication was obtained from the patient.
