ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1SHO, Neurology Department, Churruca-Visca Medical Police Hospital, Buenos Aires, Argentina; Teaching Assistant, Neurosurgery, University of Buenos Aires, Argentina.
2Consultant, Movement Disorders Unit, Neurology Department, Churruca-Visca Medical Police Hospital, Buenos Aires, Argentina.
3Consultant, Neurology Department, Churruca-Visca Medical Police Hospital, Buenos Aires, Argentina.
4Head of Neurology Department, Churruca-Visca Medical Police Hospital, Buenos Aires, Argentina.
SHO, Neurology Department, Churruca-Visca Medical Police Hospital, Buenos Aires, Argentina; Teaching Assistant, Neurosurgery, University of Buenos Aires, Argentina.
Tel: +54-9-11-3390 2036;
Email: mauriciodesampaio@gmail.com
Received : Oct 14, 2024,
Accepted : Nov 13, 2024
Published : Nov 20, 2024,
Archived : www.jclinmedcasereports.com
Introduction: Mild Encephalopathy with Reversible Splenial lesion (MERS) is a clinical-radiological spectrum characterized by acute encephalopathy due to a reversible cause associated with a transient cytotoxic lesion affecting the splenium of the corpus callosum. It is considered a benign condition due to its reversibility and excellent prognosis. MERS is characterized by altered consciousness, delirium, and seizures. The time between the prodrome and the onset of encephalopathy usually ranges from one to seven days. We present a case of MERS due to its atypical presentation.
Case presentation: A 60-year-old Caucasian female with a history of dyslipidemia and endometrial polyps presented to the emergency department with flu-like symptoms lasting 72 hours, associated with two syncopal episodes. Brain Magnetic Resonance Imaging (MRI) revealed a lesion in the splenium of the corpus callosum, with restricted diffusion on DWI and hyperintensity on FLAIR sequences without enhancement after gadolinium infusion. Additional studies, including lumbar puncture, laboratory tests, and MR spectroscopy, showed no pathological findings. A follow-up MRI performed 30 days later showed complete resolution of the lesion.
Conclusion: MERS has been classically described in children with concomitant infections, mostly viral. Increasing cases are being reported in adults. When encountering a patient with a cytotoxic lesion in the corpus callosum, MERS should be considered as a differential diagnosis; however, it is essential to rule out other etiologies with worse prognosis and specific treatments.
Keywords: Corpus callosum; Mild encephalopathy with reversible splenial lesion; Non-specific symptoms.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Emanue DSM (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Mild Encephalopathy with Reversible Splenial Lesion (MERS) is a clinical-radiological syndrome characterized by an acute encephalopathy associated with a transient cytotoxic lesion affecting the splenium of the corpus callosum [1]. It is considered a benign condition due to its reversibility and excellent prognosis in most cases. Recognizing these lesions is crucial to rule out secondary causes and avoiding misdiagnosis of ischemia. It has a prevalence of 3%, with an incidence of less than 1% in patients with encephalitis/encephalopathy and less than 6% in those with splenial lesions [2].
The recognized etiologies include viral, bacterial, and parasitic infections; toxicity or withdrawal from Antiepileptic Drugs (AEDs), and acute metabolic disorders [3].
Clinically, it is characterized by encephalopathy associated with prodromal events. The time between the prodrome and encephalopathy usually varies from one to seven days. Other neurological symptoms include neuropsychiatric manifestations, ataxia, dysarthria, and progressive impairment of consciousness, potentially leading to coma [4].
In addition to clinical findings, radiological studies are crucial for diagnosis, revealing rounded or oval lesions in the center of the splenium which either extend or not laterally or towards the anterior portion of the corpus callosum. These lesions show signal restriction on DWI, decreased signal on ADC mapping compatible with cytotoxic edema, hyperintensity on T2 and FLAIR sequences, hypointensity on T1, and no signal enhancement following gadolinium administration [1]. As the name suggests, these lesions regress over time, typically following a benign course with a favorable prognosis. This article presents a case of MERS reported at the Neurology Department of the Churruca-Visca Medical Complex, notable for its atypical presentation without signs of encephalopathy.
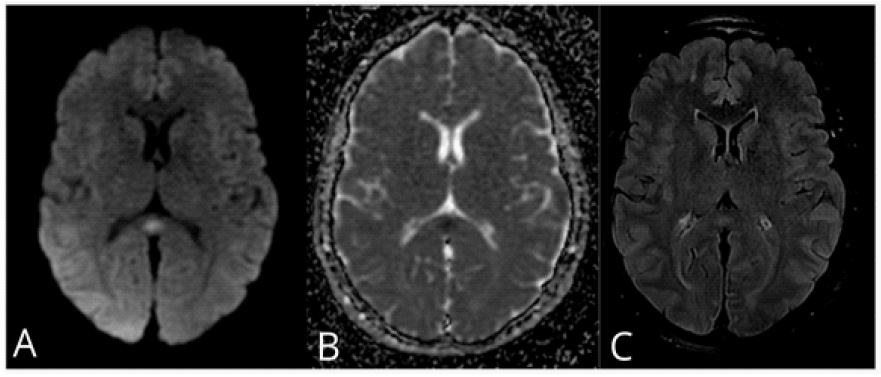
We report a case of a 60-year-old Caucasian female, with a medical history of dyslipidemia treated with rosuvastatin 10 mg/day and endometrial polyposis. In October 2022, she visited the emergency department due to a 72-hour flu-like syndrome characterized by dizziness, fever and a cough, associated with two syncopal episodes in the last 24 hours. On physical examination the patient was alert, globally oriented, with preserved speech, no dysarthria, no motor or sensory focal signs, with preserved coordination, and no signs of meningeal irritation. During the initial work-up, a brain Magnetic Resonance Imaging (MRI) revealed a rounded focal lesion at the splenium of the corpus callosum, showing restricted diffusion on DWI with decreased ADC values, and hyperintensity on FLAIR and T2 sequences without contrast enhancement, leading to her admission for further investigation and follow-up (Figure 1).
During her hospitalization she did not experience neurological findings such as seizures, disturbance of consciousness ordelirium. Laboratory tests were performed, including antibodies for rheumatologic diseases, viral serologies, and an electrophoretic proteinogram, all within normal range. Due to the nonspecific respiratory symptoms, a respiratory virus PCR panel (FilmArray©) was performed with no positive results.
A lumbar puncture was performed, showing crystal-clear cerebrospinal fluid with a protein level of 40.8 mg/dL, glucose 57 mg/dL (paired serum glucose of 94 mg/dL) and a white blood cell count of 0/mm³. Opening pressure was 12 cm H2O; cytological studies, cultures, flow cytometry, and PCR panels (viral, bacterial, and fungal - FilmArray© CSF) were normal.
An EEG did not show any epileptiform activity.
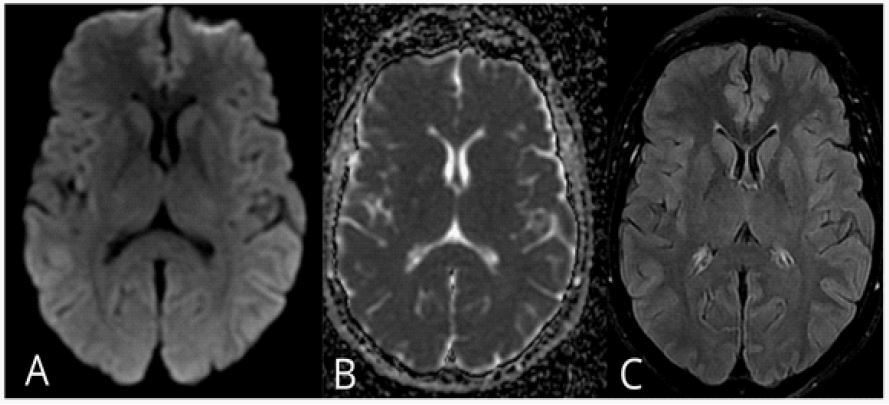
A brain MRI spectroscopy revealed normal concentrations of evaluated metabolites. Additionally, a full-body PET-CT scan showed a small, non-specific 10 mm left pulmonary opacity without pathological uptake. The clinical and radiological presentation was interpreted as compatible with MERS. To confirm this diagnosis, a follow-up brain MRI was performed 30 days later, which showed no evidence of the previously described lesion. During further follow-up the patient did not experience any new symptoms (Figure 2).
| 1. Onset with neuropsychiatric symptoms, such as abnormal speech and/or behavior, along with altered consciousness and seizures, within 1 week of the onset of fever. |
| 2. Complete recovery without sequelae within 10 days of the onset of neuropsychiatric symptoms. |
| 3. Hyperintense lesion in the splenium of the corpus callosum during the acute phase. T1 and T2 signal changes are mild. |
| 4. The lesion may symmetrically affect the entire corpus callosum and cerebral white matter. |
| 5. The lesion disappears within 1 week, with no residual signal changes or atrophy. |
In patients with MERS, encephalopathy is characterized by altered consciousness, delirium, and seizures. Patients often present with a prodromal period, most frequently characterized by fever, followed by headache, vomiting, and diarrhea [5]. In a recent meta-analysis by Chiara et al., it was shown that in a sample of 51 adult patients diagnosed with MERS 88% experienced prodromal symptoms, mainly fever (78%) and/or flu-like symptoms (42%). Headache was the most frequent presenting symptom, present in 25(50%) patients and in 10(20%), it was the only neurological symptom. Seizures and altered consciousness were present in 11(22%) patients, and delirium was observed in 8(16%) patients [6]. In the presented case, we can observe an atypical presentation of MERS compared to what is described in the literature, as there were no neurological symptoms, with only the so-called prodromal stage being present.
Since the patient was hospitalized and the diagnosis was made based on criteria that included lesion reversibility (Table 1) [7], it was necessary to pursue differential diagnoses that might require alternative therapies. Among those highlighted in the literature are lymphoma, infarction, tumors (lipoma, glioblastoma), multiple sclerosis, Marchiafava-Bignami disease, diffuse axonal injury associated with trauma, Posterior Reversible Encephalopathy Syndrome (PRES), acute encephalopathy associated with intravenous immunoglobulin treatment, alcoholism, malnutrition, and myelin disorders (Krabbe disease, X-linked adrenoleukodystrophy) [1]. However, these were clinically and radiologically ruled out in our patient.
Although the described case was not associated with a specific etiological agent, the clinical presentation of a febrile syndrome with nonspecific symptoms suggests that the pathology could be attributed to an infectious event whose etiological agent was not included in the panels available at our institution. Toxicity or withdrawal from AEDs or acute metabolic disturbances were ruled out. Reported literature indicates that up to 73% of cases have an unknown etiology, with infectious origins being the most frequently associated [6].
The pathophysiology of these reversible splenial lesions of the corpus callosum is not well understood due to the diversity of etiologies. It is possible that several mechanisms are responsible, such as intramyelinic edema, oxidative stress, autoimmuneprocesses, inflammation, cytotoxic edema characterized by swelling of neurons and glial cells with reduced extracellular space, and vasogenic edema [8].
In type 1 MERS, the lesions are limited to the splenium (oval or band-shaped), as seen in our clinical case, whereas in type 2 MERS, the lesions are not limited to the splenium. The clinical and radiological outcome is usually favorable, with clinicalimprovement occurring within 1 to 2 days, while radiological improvement occurs within 10 days to 4 months [9], although more typically the lesions resolve within two weeks. The follow up MRI in the presented case was performed one month after the initial imaging, which no longer showed the cytotoxic lesion. In rare cases, especially those with type 2 MERS lesions, neurological sequelae may develop, with type 1 lesions having the best prognosis [9].
The therapeutic approach is based on symptomatic treatment, although if an infectious agent is found, its treatment may change the prognosis [1]. Antivirals, corticosteroids, and immunoglobulins have been used, with a good response in all cases. However, their efficacy remains uncertain given the reversibility of the condition [2]. In this case presented, no specific symptomatic treatment was required.
MERS has been classically described in children with concomitant infections, mostly viral. An increasing number of cases have been reported in adults. When encountering a patient with a cytotoxic lesion of the corpus callosum, MERS should be considered as a differential diagnosis. However, etiologies with a worse prognosis and specific treatment must be ruled out. Furthermore, while the most characteristic presentation is associated with altered levels of consciousness, we present this atypical clinical case, which should be considered within the spectrum of clinical presentations of this condition.
