ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Student, Anesthesiology, Department of Anesthesiology and Intensive Care Unit, Targu Mures County Emergency Hospital, Targu Mures, Romania.
2Assistant Professor, Anesthesiology, Department of Anesthesiology and Intensive Care Unit, Targu Mures County Emergency
Hospital, Targu Mures, Romania.
3Associate Professor, Anesthesiology, Department of Anesthesiology and Intensive Care, George Emil Palade University of
Medicine, Pharmacy, Sciences and Technology, Târgu Mureș 540142, Romania.
Student, Anesthesiology, Department of Anesthesiology and Intensive Care Unit, Targu Mures County Emergency Hospital, Targu Mures, Romania.
Email: puimihai@yahoo.com
Received : Oct 12, 2024,
Accepted : Nov 18, 2024
Published : Nov 25, 2024,
Archived : www.jclinmedcasereports.com
Background: Pneumorachis, the presence of air within the spinal canal, is a rare clinical condition. This case report describes a patient with pneumorachis associated with septic shock due to mesenteric infarction.
Case presentation: A 67-year-old male presented obnubilated, hypotensive, and hyperglycemic. Imaging revealed mesenteric infarction, pneumoperitoneum, and pneumorachis along with additional findings.
Conclusion: This case highlights the importance of recognizing pneumorachis and understanding its potential causes and implications for patient management.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Claudiu PM (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Pneumorachis, defined as the presence of air within the spinal canal, is an exceptionally rare clinical finding typically associated with traumatic or iatrogenic causes. This condition can manifest as either epidural or subarachnoid air, with the former being more common due to its proximity to potential entry points for air, such as fractures or surgical sites. The occurrence of pneumorachis in the context of septic shock, however, is particularly unusual and warrants attention due to its implications for patient management and outcomes [1,2].
Septic shock is a severe and life-threatening response to infection, characterized by profound circulatory, cellular, and metabolic abnormalities. It often follows severe infections such as mesenteric infarction, where the loss of blood supply to the intestines leads to extensive tissue necrosis and subsequent infection. Gas-forming organisms, such as certain anaerobic bacteria, can thrive in these necrotic tissues, producing gas that may track along fascial planes and enter the spinal canal [1,2].
Mesenteric infarction itself is a critical condition that typically presents with acute abdominal pain and can rapidly progress to peritonitis and septic shock if not promptly diagnosed and treated. The combination of mesenteric infarction and septic shock creates a highly complex clinical scenario, with the added complication of pneumorachis further complicating the clinical picture [3].
This case report presents a 67-year-old male who developed pneumorachis in the setting of septic shock secondary to mesenteric infarction. The aim is to highlight the rare association between pneumorachis and septic shock, explore the pathophysiological mechanisms underlying this link, and discuss the diagnostic and therapeutic challenges encountered. Through this case, we emphasize the importance of a comprehensive diagnostic approach and timely intervention to improve patient outcomes in complex and life-threatening scenarios.
A 70-yearon,
A 67-year-old male with no significant pathological history was found at home obnubilated, hypotensive, and hyperglycemic and with severe pain. The patient was urgently transported to the hospital.
On presentation
• Low blood pressure (71/46 mmHg) and hypoperfusion (capillary refill time >3s)
• Tachycardia (114 bpm)
• Severe abdominal pain and absence of bowel sounds
• Fever (38.9 Celsius degrees)
• Lack of diuresis, indicative of Acute Kidney Injury (AKI) stage III
• Liver failure
• Thrombocytopenia
• Hyponatremia
• Hyperkalemia
Initial diagnosis
The initial clinical assessment suggested an acute abdomen due to the patient’s clinical exam and severe pain.
Initial management
• Fluid resuscitation: The patient received aggressive fluid resuscitation with crystalloids.
• Vasopressors and inotropes: Initiation of Dobutamine (10 mcg/kg/min) and Noradrenaline (0.8 mcg/kg/min) to support blood pressure and cardiac output.
• Antibioterapy: Initiation of empirical broad-spectrum antibiotics. (Meropenem 2x500 mg and Metronidazol 3x500 mg)
• Analgesic drugs: 1 g of Acetaminophen, 1 g of Metamizole, and 2 mg of subcutaneous Morphine.
Imaging studies: An initial Computed Tomography (CT) of the head, thoracic, and cervical spine demonstrated:
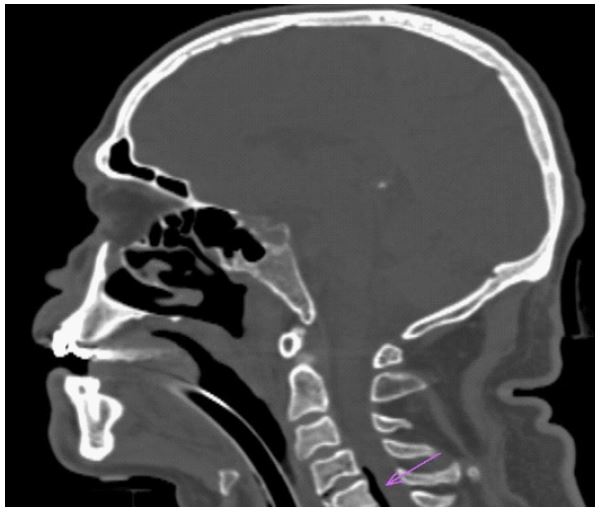
Head and cervical spine: Marked diffuse bihemispheric cerebral edema, with obscuration of gyri.
The hyperdense appearance of the afferent and efferent arteries of the circle of Willis and at the intergyral fronto-parietal bilateral level, the imaging appearance suggests pseudo-subarachnoid hemorrhage (pseudo-SAH). Obliteration of the mesencephalic cisterns. Spheno-maxillary-ethmoidal sinusitis. Cervical pneumorachis (Figure 1).
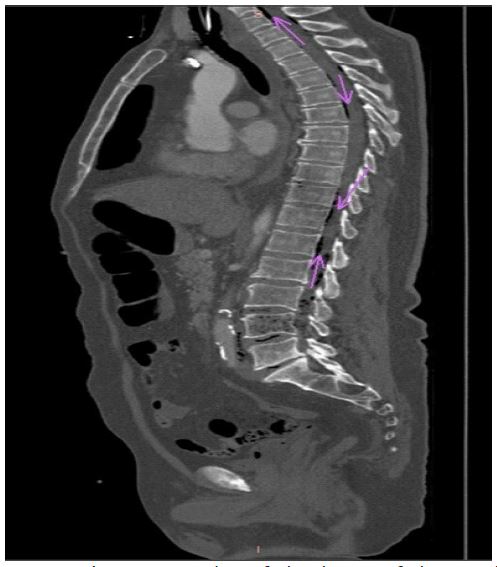
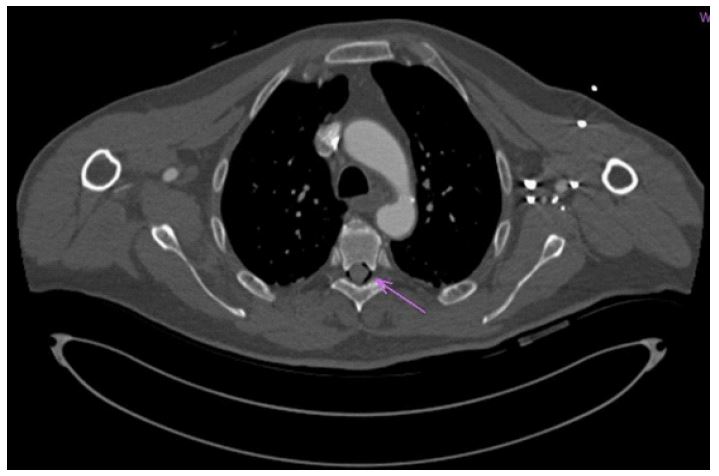
Thoracic: Minimal pericardial fluid ventral to the position of the heart (13 mm). Thoracic pneumorachis (Figures 2 & 3). Abdomen and lumbar: Bilateral pneumoperitoneum, more extensive on the right side. aeroportia, with distal aero mesentery, secondary to hypo opacification of some intestinal loops located at the pelvis level, immediately cranial to the urinary bladder.
Work-up diagnostic
| Test | Results | Reference range |
|---|---|---|
| Leukocyte count | 18.73 ↑ | 3.6-10 (103 muL) |
| Erythrocyte count | 4.11 ↓ | 4-6 (106 muL) |
| Hemoglobin | 12.7 ↓ | 13-17 (g/dL) |
| Hematocrit | 37.7 ↓ | 39-54 % |
| Platelet count | 41 ↓ | 150-450 (103muL) |
| Neutrophils | 17.19 ↑ | 1.4-6.5 (103/muL) |
| Lymphocytes | 0.81 ↓ | 1.2-3.4 (103/muL) |
| Prothrombin Time | 24.8 ↑ | 9.9-12.3 |
| INR | 1.96 ↑ | 0.91-1.16 |
| APTT | 39.6 ↑ | 1.6-28.7 |
| Albumin | 1.70 ↓ | 3.97-4.94 (g/dL) |
| ALT | 513.00↑ | 0-41 (U/L) |
| Amylase | 781.00↑ | 28-100 (U/L) |
| AST | 1654.00 ↑ | 0-40 (U/L) |
| Direct Bilirubin | 1.04 ↑ | 0-0.3 (mg/dL) |
| Creatine Kinase | 15184.00 ↑ | 38-190 (U/L) |
| Creatinine | 4.56 ↑ | 0.7-1.2 (mg/dL) |
| eGFR (calculated) | 13.75 ↓ | >60 (ml/min) |
| C-Reactive Protein | 387.00↑ | 0-0.5 (mg/L) |
| Glucose | 136.00↑ | 70-99 (mg/dL) |
| Lactate Dehydrogenase | 2012.00 ↑ | 0.5-214 (U/L) |
| Urea | 185.00↑ | 18-55 (mg/dL) |
INR- International Normalized Ratio, APTT- Activated Partial Thromboplastin Time, ALT- Alanine Aminotransferase, AST- Aspartate Aminotransferase, GFR-Glomerular Filtration Rate. Values indicated ↑ are above the reference range, and those indicated ↓ are below the reference range.
At the peripheral level, the branches supplying the described loops show serial defects, with a severe reduction in arterial density - entero-mesenteric infarction. Severe benign character stenosis at the splenic flexure of the colon. Lumbar pneumorachis (Figure 4).
Surgical intervention:
• Extended resection of the ileum
• Wide right hemicolectomy
• Mechanical side-to-side ileum-transverse anastomosis
• Intraoperative microbiological sampling
Postoperative management:
• Admission to the Intensive Care Unit (ICU)
• Antibiotic therapy: Adjusted after results of intraoperative sampling came positive for Escherichia coli (Meropenem 3x500 mg.)
• Hemodynamic status: Continued instability despite supportive measures
| Parameter | Value | Units | Reference range |
|---|---|---|---|
| pH | 7.17 | - | 7.35-7.45 |
| pCO₂ | 43 | mmHg | 35-48 |
| pO₂ | 119 | mmHg | 83-108 |
| Na⁺ | 130 | mmol/L | 135-145 |
| K⁺ | 5.9 | mmol/L | 3.5-5.1 |
| Cl⁻ | 108 | mmol/L | 98-107 |
| Ca²⁺ | 0.88 | mmol/L | 1.15-1.27 |
| HCO₃⁻ | 19 | mmol/L | 20-29 |
| Glu | 135 | mg/dL | 70-105 |
| Lac | 2.0 | mg/dL | 0.3-1.2 |
| sO₂ | 100 | % | 95.0-98.0 |
| BE | -8.5 | mmol/L | -3.0-3.0 |
| AG | 17 | - | 10-18 |
| P/F Ratio | 72 | - | - |
pH: power of hydrogen; pCO2: the partial pressure of carbon dioxide; pO2: the partial pressure of oxygen; Na: sodium; K: potassium; Cl: chloride; Ca: calcium; HCO3: bicarbonate; Glu: glucose; Lac: lactate; sO2: saturation of oxygen; BE: base excess; AG: anionic gap; P/F Ratio: ventilation/perfusion ratio.

• Culture results: Intraoperative fluid culture positive for Escherichia coli
Outcome: Shortly after ICU admission, the patient’s condition deteriorated, and he succumbed to the severe complications of septic shock.
Pneumorachis is a rare clinical finding often associated with trauma or iatrogenic causes. Its occurrence in the context of septic shock due to mesenteric infarction is particularly unusual and highlights the severity of the patient’s condition. The presence of air within the spinal canal, pneumoperitoneum, aeroportia, and aeromesenteria indicates a severe systemic infection with gas-forming organisms. These bacteria can produce gas that migrates along tissue planes into the spinal canal, exacerbating the clinical scenario [4,5].
The pathophysiology of pneumorachis in septic shock likely involves the migration of gas produced by anaerobic bacteria from necrotic intestinal tissues into the retroperitoneal space and subsequently into the spinal canal [5]. This can occur through natural anatomical pathways or due to the breakdown of tissue barriers during severe inflammation and infection. Association between pneumorachis and septic shock due to mesenteric infarction could be:
Infection and gas formation: In the context of mesenteric infarction, necrotic bowel tissue can become infected with gas-forming organisms. These bacteria can produce gas as a byproduct of their metabolism [1,2,4-7].
Gas dissemination: The produced gas can then disseminate through tissue planes, potentially reaching the spinal canal and leading to pneumorachis. This is especially plausible in cases where the infection is severe and spreads rapidly, compromising multiple structures [1,2,4-8].
Increased intra-abdominal pressure: Septic shock often involves fluid resuscitation and other treatments that can increase intra-abdominal pressure. Increased pressure can force air into the vascular system or through tissue planes into the spinal canal.
Direct invasion: In severe septicemia, bacteria, and gas can invade the bloodstream and disseminate to various body parts, including the spinal canal, leading to pneumorachis [1,2,4-8].
Early recognition and diagnosis are crucial in managing such complex cases effectively. Angio-CT imaging plays a vital role in identifying the extent of pathology, including signs of mesenteric infarction, pneumoperitoneum, and pneumorachis [6-9]. The importance of comprehensive diagnostic evaluation cannot be overstated, as timely intervention is critical to improving patient outcomes [6-10].
Management of these patients involves a multidisciplinary approach, including aggressive fluid resuscitation, vasopressor and inotropic support, broad-spectrum antibiotics, and prompt surgical intervention. Despite these measures, the prognosis remains poor in cases with extensive tissue necrosis and severe systemic infection, as evidenced by the rapid deterioration and eventual death of the patient in this report [3,7-10].
This case illustrates the importance of a comprehensive diagnostic approach and timely intervention in patients presenting with septic shock and complex intra-abdominal pathology. Early imaging and surgical intervention are essential to identify and treat the underlying cause, prevent further complications, and improve survival rates. The high mortality rate associated with non-occlusive mesenteric ischemia and septic shock underscores the aggressive nature of these conditions and the need for rapid and effective treatment strategies [7-10].
This case report highlights the rare occurrence of pneumorachis associated with septic shock due to mesenteric infarction. The presence of pneumorachis in this context underscores the severity of the underlying condition and the systemic spread of gas-forming bacteria. Early recognition, comprehensive diagnostic evaluation, and prompt intervention are crucial in managing such complex cases. Despite aggressive treatment, the prognosis in cases of septic shock with multi-organ failure remains poor. This case emphasizes the importance of a multidisciplinary approach and the need for continued vigilance in patients presenting with severe abdominal pain and signs of systemic infection to improve outcomes and reduce mortality.
By reporting this case, we aim to increase awareness of this rare but serious complication and highlight the critical need for early and effective management strategies in similar clinical scenarios.
Ethics statement: The study involving human participants was registered and approved by the Ethics and Clinical Drug Study Ethics Committee of the Targu Mures County Emergency Hospital (reference number: 18817/27.08.2024). Written informed consent has been obtained from the person’s legal guardian for the publication of any potentially identifiable images or data included in this article.
