ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Resident, Dento-Facial Orthopedics Department of Farhat Hached Hospital, Sousse, Laboratory of Oral Health and Orofacial Rehabilitation, Tunisia.
2Head, Dento-Facial Orthopedics Department of Farhat Hached Hospital, Sousse, Laboratory of Oral Health and Orofacial Rehabilitation, Tunisia
esident, Dento-Facial Orthopedics Department of Farhat Hached Hospital, Sousse, Laboratory of Oral Health and Orofacial Rehabilitation, Tunisia.
Email: ines.medhioub18@gmail.com
Received : Nov 14, 2024,
Accepted : Dec 11, 2024
Published : Dec 18, 2024,
Archived : www.jclinmedcasereports.com
Adult patients seeking orthodontic treatment consistently have aesthetic concerns, even throughout the course of the treatment. This has lead to the introduction of Lingual Orthodontics in 1970s by Dr. Craven Kurz of USA and Dr. Kinya Fujita of Japan. Lingual orthodontics, in addition to its aesthetic benefits, offers several other advantages. The cooperation and confidence level of the patient has increased with the invisible appliances. The Anchorage control, indirect bonding and biomechanics is completely different from labial technique. In this article the concept of lingual orthodontics has been highlighted.
The article shows a case report with lingual technique treated in the department of orthodontics at Farhat Hached University Hospital.
Keywords: Lingual orthodontic; Adult treatment; Invisible appliance
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cao G (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Lingual orthodontics is a specialized approach to orthodontic treatment that uses brackets and wires placed on the lingual surfaces of the teeth, providing a fully discreet and aesthetic solution for patients seeking orthodontic correction without visible appliances. Introduced in the 1970s by pioneers like Kurz and Fujita, lingual orthodontics has evolved significantly, incorporating advanced materials and techniques that allow for more precise and comfortable treatment. Modern lingual systems, such as the customized Incognito and prefabricated In-Ovation L, offer a range of options tailored to the needs of the patients, from mild crowding to complex malocclusions.
The primary advantage of lingual orthodontics is its invisibility, which makes it particularly appealing to adults and those concerned with the aesthetic impact of traditional braces. However, the technique requires a high level of skill, both in bracket placement and wire adjustments, due to the difficulty in accessing the lingual surfaces. Additionally, lingual appliances may pose challenges in terms of patient comfort, speech, and oral hygiene, especially during the initial stages of treatment.
Despite these challenges, lingual orthodontics offers several benefits, including reduced visibility, fewer aesthetic compromises, and the ability to treat a wide range of malocclusions, from mild crowding to more complex skeletal discrepancies. Furthermore, the integration of digital technologies in bracket design and customization has significantly enhanced the precision and predictability of lingual treatments.
This article reviews the principles of lingual orthodontics, discusses its clinical applications, and explores the advancements that have shaped this treatment modality. It also examines patient outcomes, highlighting both the advantages and limitations of lingual appliances in achieving functional and aesthetic goals in orthodontic treatment [1].
• Aesthetic appeal: Lingual braces are placed on the inner surface of the teeth, making them nearly invisible from the outside. This is ideal for patients who want to straighten their teeth without the visible appearance of traditional braces.
• Discreet treatment: Since lingual braces are hidden behind the teeth, they are a popular option for adults and professionals who may feel self-conscious about wearing traditional braces.
• Effective for all ages: Lingual braces can be used to treat both adults and children, making them suitable for a wide range of orthodontic cases [2].
• The cost difference is significant; lingual braces are 3 to 4 times more expensive than vestibular treatments.
• The discomfort associated with this treatment is more pronounced compared to vestibular braces, as it may interfere with the natural movement of the tongue.
• Risk of tongue injury.
• Very delicate positioning of the brackets in direct bonding technique [2].
Lingual orthodontics offers the same potential for controlling dental movements as vestibular orthodontics. This technique is suitable for treating minor dental misalignments, complex cases requiring the extraction of permanent teeth, and orthognathic (surgical orthodontics) cases.
The patient is a 22-year-old woman who consulted the orthodontic unit at CHU Farhat Hached Sousse for aesthetic reasons (maxillary and mandibular crowding).
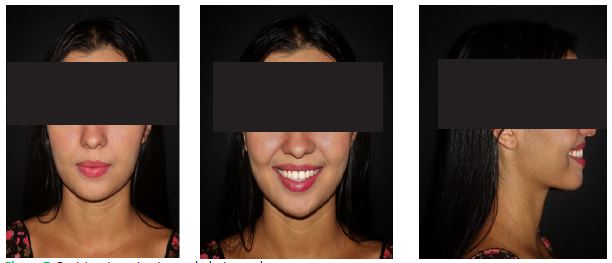
The extraoral frontal examination shows parallelism between the ophryal, bipupillary, and bicommissural lines, with an increased lower facial height.
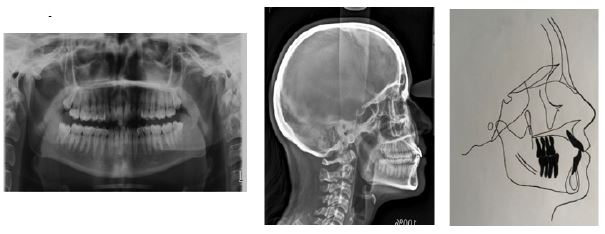
The extraoral lateral examination reveals a convex profile with a frontally aligned forehead, a straight nasal ridge, a normal nasolabial angle, and a cervicomental distance of four of the patient’s fingers (Figure 1).
The intraoral examination reveals U-shaped arches, with a Class I molar and canine relationship on both the right and left sides, along with anterior crowding in both the upper and lower arches. There is also a deviation of the lower midline towards the left side (Figure 2).
The radiological assessment includes
Cephalometric analysis (Table 1) and tracing showed class 1 skeletal relationship (ANB= 1°, AoBo=-1mm), proclination of the upper and lower incisor (I/F=118° , IMPA = 105°), and short facial height (FMA= 19°).






| SNA | 79° |
|---|---|
| SNB | 78° |
| ANB | 1° |
| Ao Bo | -1mm |
| FMA | 19° |
| FMIA | 56° |
| IMPA | 105° |
| I/i | 117° |
| I/F | 118° |
| Z | 75° |
| + | - | |
|---|---|---|
| Enc | 8 | |
| RI | 8 | |
| C Spee | 2 | |
| DDM | 18 | |
| Exo | 16 | |
| NET | 2 |
The patient presents with a skeletal Class I malocclusion combined with facial hypodivergence. On the dentoalveolar level, she has a Class I molar and canine relationship with proclined upper and lower incisors.
Resolution of dental crowding.
To maintain class I canine and molar relationships.
Establishment of a functional overjet and overbite.
Correction of the arch form.
To achieve optimal facial esthetics.
A non-extraction orthodontic treatment with lingual appliance was our treatment of choice.
Before starting orthodontic treatment, the patient was referred to a periodontist for probing, evaluation and initial therapy including motivation to oral hygiene and supragingival plaque control.
Then, orthodontic treatment using the 2D system (Innovation L brackets from GAC) was initiated with direct bonding technique.
Bracket Bonding (Figure 4).
Here’s an overview of the direct bonding process for lingual orthodontic treatment:
1. Preparation
• Oral hygiene: The patient’s teeth are thoroughly cleaned, and any plaque or tartar is removed to ensure proper bonding.
• Isolation: The teeth are isolated using cotton rolls or cheek retractors to keep the treatment area dry, which is essential for successful bonding.
2. Etching
• The lingual surfaces of the teeth are etched with a phosphoric acid gel to create micropores for better adhesion of the bracket.
3. Bonding
• A bonding resin is applied to the etched surfaces of the teeth.
• The orthodontist then places the brackets directly on the lingual surfaces of the teeth, ensuring proper positioning according to the treatment plan.
The upper and lower arches were bonded and 0.012 NITI wire was inserted for initial leveling.
Then, a NITI 0.014, 0.016, 0.018 was used.
The overall active treatment time was 16 monthes.
After debonding of the lingual appliance, fixed retainers were placed in both arches to maintain Long-term stability (Figure 8).
After 6 months of treatment, the space was opened for the 31 using a compressed spring (Figure 5).
After 12 monthes, the 31 was placed, and maxillary and mandibular leveling was achieved (Figure 6).
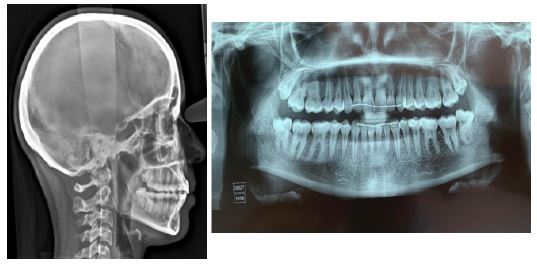
The final extraoral photographs show the restoration of facial aesthetics. The patient’s smile and profile are now more harmonious (Figure 7).
Final radiographic assessment
The panoramic radiograph shows no evidence of root proximity.
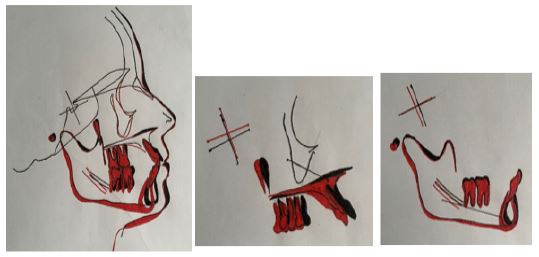
The cephalometric analysis, along with both local and general superimpositions, reveals a slight lower alveolar protrusion compared to the start of treatment (Figures 9 & 10).
In recent years, the growing number of adult patients seeking orthodontic treatment and their higher aesthetic expectations have led to the development of various cosmetic treatment approaches, including aesthetic brackets (Innovation C by GAC, Damon Clear, etc.) and clear aligners (Invisalign, Smilers, etc.). While these reduce the visual presence of the appliance, they remain visible, which is still a concern for some patients [1].
In this regard, lingual orthodontics represents the ideal solution due to its complete discretion.
Since the introduction of lingual appliances by FUJITA, advancements have been made in their design and fabrication. The benefits of lingual appliances offered by clinicians or manufacturers include reduced visibility, fewer carious lesions and white spots, lighter forces due to a smaller inter-bracket distance, less anchorage loss, and increased comfort [2,4].
There are several systems available on the market, including customized options such as the Liberty, Incognito, and Win systems, which are now considered benchmarks in the field of new-generation technologies, with proven efficacy in adult lingual orthodontics [7,8].There are several systems available on the market, including customized options such as the Liberty, Incognito, and Win systems, which are now considered benchmarks in the field of new-generation technologies, with proven efficacy in adult lingual orthodontics [7,8].
There are also prefabricated systems, such as the In-Ovation L by GAC, which is the system we used to treat our patient.
In-Ovation L is a two-dimensional self-ligating lingual system that does not take into account the third order. It features a true bi-plot design with an optimal mesio-distal distance, offering enhanced control of rotation, and a spring-loaded interactive clip that can function in a passive, interactive, or active role, allowing for optimal control of the arch engagement throughout all treatment phases.
The In-Ovation L system is typically used for patients with interdental diastemas or mild dental crowding, which was the case for our patient, who presented with a skeletal Class I, a Class I molar and canine relationship on both sides, anterior maxillary and mandibular crowding, and proclined upper and lower incisors [9].
The patient sought orthodontic treatment but refused visible braces, so we proposed fixed orthodontic treatment using the lingual technique with the In-Ovation L system by GAC [1,5].
After bonding, stripping was performed and a bite block was placed to prevent bracket detachment during closure movements. Then, prefabricated “mushroom” archwires were inserted.
In lingual orthodontics, direct bonding and indirect bonding refer to two different methods of attaching the brackets to the teeth. Both methods are effective, but they each have distinct advantages and challenges. Below is a comparison of direct bonding vs. indirect bonding in lingual orthodontics.
Direct bonding in lingual orthodontics
Process: Direct bonding involves the orthodontist attaching the brackets directly to the teeth during the appointment. This method requires the orthodontist to individually place each bracket on the inner surface of the tooth and bond it using dental adhesive.
Indirect bonding in lingual orthodontics
Process: Indirect bonding involves a multi-step process where an impression or digital scan of the patient’s teeth is taken first. From this, a model of the teeth is created in a lab. The brackets are then bonded to the model of the teeth, and a custom transfer tray is fabricated. This tray is used to transfer the bonded brackets onto the patient’s teeth in a second appointment.
Which is better?
Direct Bonding may be more appropriate for patients with simpler orthodontic needs, where the orthodontist can place the brackets quickly and effectively, or when cost is a concern. It is also beneficial for cases where time is of the essence, and the orthodontist can directly modify the bracket placement on the spot.
| Feature | Direct Bonding | Indirect Bonding |
|---|---|---|
| BracketPlacement | Brackets are placed directlyon the teeth. | Brackets are placedon amodel beforetransfer. |
| Time in Chair | Longer due to individual bracketplacement. | Shorterdue to pre- bonding on a model and tray. |
| Precision | Dependent on orthodontist'sskill, prone to errors. | Greater precision since brackets are pre- positioned. |
| Comfort | Potentiallyuncomfortable due to prolonged mouth opening. | Morecomfortable for the patient with fewerindividual steps. |
| Laboratory Involvement | Low, as no model or transfer tray is required. | High, requiring custom models and transfer trays. |
| Cost | Generally lower due toless lab involvement. | Higher, due to lab feesand the multi-step process. |
| Patient Follow-up | None needed for bracket placement; focus on adjustments. | Requires extra time for the fabrication of models and trays. |
| Flexibility | More adaptable during the procedure. | Less flexibility once brackets are placed on the model. |
Indirect Bonding is generally preferred for more complex cases or when precise, customized bracket placement is necessary. It is particularly useful for patients with more severe malocclusion or those who need very accurate bracket positioning to achieve optimal results. This method also minimizes patient discomfort during the bracket bonding phase [3].
The choice between direct bonding and indirect bonding in lingual orthodontics largely depends on the complexity of the case, the desired level of precision, patient comfort, time constraints, and budget. Both methods are effective, but indirect bonding tends to be the go-to choice for more precise, efficient, and comfortable treatment in more complex cases.
