ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Department of Midwifery, School of Nursing and Midwifery, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia.
Department of Midwifery, School of Nursing and Midwifery, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia.
Email: datrsaw2006@gmail.com
Received : Nov 17, 2024,
Accepted : Dec 16, 2024
Published : Dec 23, 2024,
Archived : www.jclinmedcasereports.com
Introduction: Postpartum Hemorrhage (PPH) is a leading cause of maternal mortality, accounting for approximately one-third of all pregnancy-associated deaths worldwide. Nonpneumatic Anti-Shock Garments (NASGs) have been endorsed for managing PPH and hypovolemic surprises, yet their adoption in sub-Saharan Africa remains suboptimal.
Objective: To assess NASG utilization rates and identify factors hindering its adoption among healthcare providers in sub-Saharan Africa.
Methods: A systematic review and meta-analysis were performed following the PRISMA guidelines. The database searches retrieved 18 observational studies from sub-Saharan Africa that were published in English. The NAGG utilization rates were pooled, and factors associated with its use were examined.
Results: The overall percentage of patients who used NASG was 37%. Subgroup evaluation revealed the highest costs among recent studies and people with smaller sample sizes. NASG use has become notably associated with more issuer expertise, preceding training, and effective attitudes in the direction of NASG.
Conclusion: Although NASG adoption for PPH management in sub-Saharan Africa has increased, it remains suboptimal. Improving company expertise, training possibilities, and perceptions of NASG represents a practical strategy to facilitate its wider uptake and reduce preventable maternal mortality.
Keywords: Nonpneumatic antishock garment; Utilization; Associated factors; Sub-Saharan Africa.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Dessie Liyew A (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Postpartum Hemorrhage (PPH) represents a significant contributor to maternal morbidity and mortality, particularly in Africa and Asia, where it bills approximately one-third of all pregnancy-related fatalities. Primary PPH is conventionally characterized by excessive bleeding of 500 milliliters or more from the genital tract within the initial 24 hours following childbirth [1,2]. Mortality is particularly high in the immediate postpartum period, with Postpartum Hemorrhage (PPH) accounting for 30% to 50% of maternal deaths [3].
Mortality from PPH is closely related to both bleeding duration and volume, and a blood loss of 40% results in hypovolemic shock, multiorgan dysfunction, global hypoxia, and severe metabolic damage; irreversible hypothermia, coagulopathy, and metabolic acidosis cause seizures (the triad of deaths) [4].
In low-income countries, many women give birth in nonclinical settings with their own family members or traditional birth attendants, increasing the danger of failing to discover early complications, potentially leading to substantial mortality within 2 hours for girls with PPH, as delays in determining which to seek healthcare facility help and limited transportation options can in addition exacerbate the state of the situation [5].
According to the FIGO/ICM guidelines, active management of the third stage of labor is crucial for reducing severe postpartum hemorrhage caused by uterine atony. This involves administering uterotonic prophylaxis and additional treatment when necessary. However, despite these measures, many women continue to experience intractable postpartum hemorrhage due to other obstetric factors. This approach may require multiple blood transfusions and even surgery, which may only be available at specialized tertiary care centers. This highlights the pressing need for effective strategies and technologies to manage obstetric hemorrhage and hypovolemic shock until comprehensive emergency obstetric care is universally accessible [6]. In situations where resources are limited and there is a delay in addressing Postpartum Hemorrhage (PPH), providing immediate aid is crucial to stabilizing women and increasing their chances of survival while awaiting definitive treatment [5].
The NASG is a simple but powerful tool that can save women’s lives during childbirth. By applying pressure to the lower body, blood is redirected to vital organs, effectively countering the dangerous effects of hypovolemic shock and reducing the risk of excessive bleeding. This can have a significant impact on women who may experience delays in receiving essential emergency obstetric care by increasing blood pressure, improving blood flow, and stabilizing vital signs. In brief, the NASG offers a low-tech solution with potentially life-saving results in obstetric emergencies [7-9].
The NASG is an innovative tool that enhances perineal accessibility and expands the abdomen, allowing for better evaluation of the uterus and improved access to arm veins for fluid administration. It has been proven effective for up to 48 hours, potentially eliminating the need for emergency hysterectomy in patients with intractable uterine atony and decreasing the necessity for blood transfusions [10].
Numerous organizations, including the FIGO, WHO, and various PPH guidelines, have wholeheartedly endorsed the use of the NASG. Additionally, a WHO healthcare technology assessment gave it a glowing endorsement, and in 2015, a collaborative effort was launched to significantly reduce the cost of the NASG by 75% to make it more accessible for utilization in low- and middle-income countries [11].
In 2012, the World Health Organization (WHO) recognized the Nonpneumatic Anti-Shock Garment (NASG) as a crucial tool for addressing Postpartum Hemorrhage (PPH) on a global scale. However, despite its potential to save lives, the NASG has faced challenges in being widely adopted and utilized. Limited awareness, high costs, and insufficient support from funding initiatives have all contributed to its limited use. Fortunately, many healthcare facilities in sub-Saharan Africa have successfully integrated the NASG into their practices, resulting in significant reductions in maternal mortality rates. Recognizing its impact, the United Nations Children’s Fund (UNICEF) included the NASG in its product innovation portfolio in 2019, opening up opportunities for its widespread availability and accessibility [12-15].
Therefore, the primary aim of this study was to assess the extent to which the NASG was utilized and to identify the factors that hindered its adoption by healthcare providers in maternal healthcare facilities in sub-Saharan Africa.
The goal of this systematic overview and meta-analysis was to determine the utilization of nonpneumatic antishock garments and associated factors among obstetric care providers in sub-Saharan Africa via the use of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist as a guideline [16].
Search strategy
We performed a scientific evaluation and meta-analysis of articles on the use of nonpneumatic anti-shock garments among obstetric care companies in sub-Saharan Africa. We searched several online databases, such as PubMed, EMBASE, HINARI, Google Scholar, Semantic Scholar and African Journal, using tailored PICO questions to obtain all vital articles.
Inclusion and exclusion criteria
We carried out a systematic overview and meta-analysis of observational studies (cross-sectional, case‒control, and cohort studies) performed in sub-Saharan Africa and published best in English. We investigated the use, utilization and associated factors of nonpneumatic anti-shock garments as a selection-making tool among health care providers. We also protected each published and unpublished study at any time. However, we excluded studies that were available most effectively as abstracts with uncertain results, commentaries, editorials, critiques, or qualitative research.
Quality assessment
After the findings were collected from all the databases and websites, the articles were exported to a Microsoft Excel spreadsheet. Three authors (ADL, NA and MA) independently extracted the facts and reviewed the screened and eligible articles. Any confrontation was addressed with the aid of 2 reviewers (ADL and NAM). Finally, a consensus was reached among the three authors through discussion. The methodological first-class of each study (sampling approach, reaction charge, and representativeness of the look at), comparability, and outcome were checked using the Joanna Brigg Institute (JBI) tool [17]. The JBI for cross-sectional and cohort research was used to evaluate the methodological significance of a study and to determine the volume at which a study was examined, addressing the possibility of bias in its design, behavior, and analysis (Supplementary Table 1).
Measurement outcomes
The study had two primary outcome variables: The utilization of Nonpneumatic Anti Shock Garment (NASG) was the first, while the second was the factor that influenced the utilization of NASG. The odds ratio was calculated for the common factors of the reported studies. This study aimed to focus on single studies that estimated the utilization of NASG.
Publication bias and heterogeneity
The study used the Cochrane Q test and I2 test with corresponding p values to assess study heterogeneity. Heterogeneity was categorized as low, medium, or high, with values of 25%, 50%, and 75%, respectively. The presence of publication bias was assessed using funnel plots. Consequently, the random effects model in the study was estimated by the amount of heterogeneity.
Search outcomes
Researchers have searched various databases and websites for 168 studies. After the records were exported to Endnote 20 Reference Manager for screening, 151 studies were excluded from the analysis because of inappropriate titles, replication findings, or distinct effects of hobbies. Finally, eighteen studies that met the inclusion criteria were included in the evaluation (Supplementaty Figure 1).
Characteristics of the included studies
To estimate the pooled stage of NASG utilization for the treatment of postpartum hemorrhage in sub-Saharan Africa, eighteen studies were included [15,18-27,29-31,33-35]. Seventeen of the included studies were cross-sectional, while one was a retrospective cohort study [35] (Supplementary Table 2).
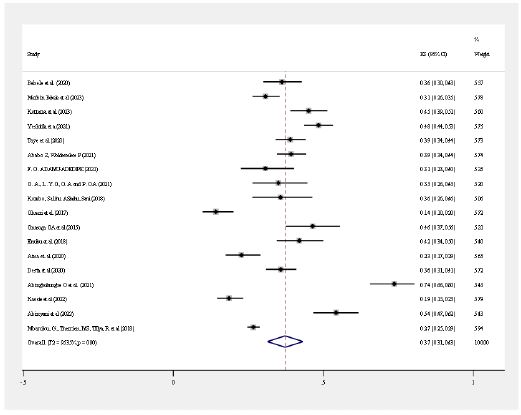
Pooled estimates of NASG utilization
The overall NASG use rate was 37%, with a confidence interval of 31-43% at the 95% confidence level. A random effects model was used to calculate the overall rate of NASG use and its corresponding confidence interval (Figure 1).
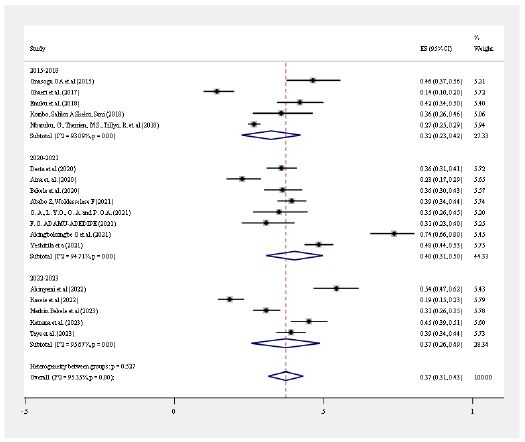
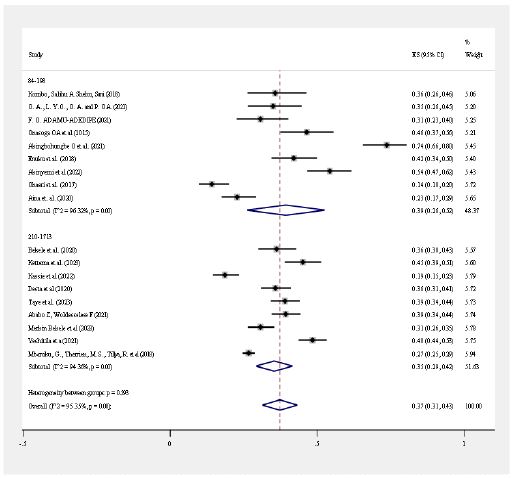
Subgroup Analysis
In this meta-analysis, we found significant heterogeneity (I2 = 95.35%, p value < 0.001) among the included studies. Due to considerable heterogeneity, subgroup analysis was performed based on the publication year and sample size of the study. The highest prevalence of NASG utilization was observed among those who were published between 2020 and 2021, at 40% (95% CI: 31–50, I2=94.71%, P<0.001), and the lowest was between 2015 and 2018, at 32% (95% CI: 23–42, I2=93.03%, P<0.001) (Figure 2a). Based on the sample size, the samples were divided into two groups according to 84-198 and 210-1713. Subgroup analysis was subsequently performed, and the highest prevalence of NASG utilization was observed for those catagorized from 84-198, which was 39% (95% CI: 26-52, I2=96.32%, P<0.001) (Figure 2b).
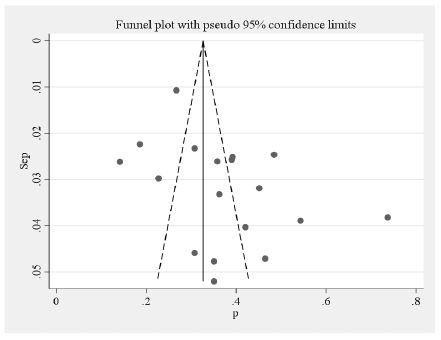
Publication bias or small study effects
The authors used a funnel plot to check for publication bias in the included studies. Funnel plots revealed a fairly even disdistribution of studies across the plot, with larger analyses concentrated near the mean effect size and smaller analyses evenly scattered above and below the median. These consistent funnel plots indicate the absence of publication bias, indicating that neither positive nor negative statistically significant findings were preferentially published and that the included publications represented an unbiased sample in terms of overall effect sizes (Figure 3).
Factors associated with NASG utilization
In this systematic review and meta-analysis, we examined the associations of factors (training status, knowledge about the NASG and attitudes toward the application of the NASG) that were significantly associated with the use of the NASG for the management of postpartum hemorrhage.
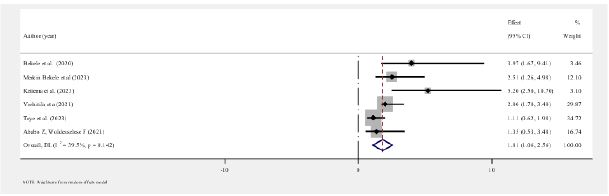
The association between the knowledge of health care providers about NASG and the utilization of NASG for PPH management
Six primary articles revealed that having a good understanding of NASG was significantly associated with its use for the management of postpartum hemorrhage [18-23]. Health care providers who had good knowledge about NASG were 1.81 (OR=1.81, 95% CI=1.06-2.56) times more likely to utilize NASG for managing postpartum hemorrhage than were those who had poor knowledge (Figure 4a).
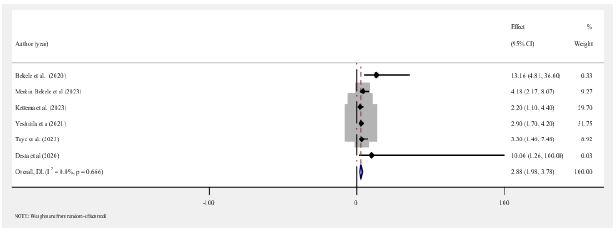
The association between the training status of health care providers about NASG and the utilization of NASG for PPH management
Among the included studies, six primary articles reported that having a health care provider who had received training in NASG was significantly associated with its utilization for the management of postpartum hemorrhage [15,18-22]. Among the health care providers who had received training on the NASG, nearly three times more utilized the NASG than did those who did not receive training (OR=2.88, 95% CI: 1.98-3.78) (Figure 4b).
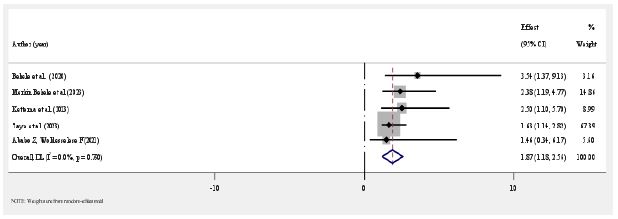
The association between the attitudes of health care providers toward the NASG and the use of the NASG for PPH management
Five primary studies from the included articles showed that health care providers who had positive attitudes toward NASG were significantly more likely to have positive attitudes toward it in the management of postpartum hemorrhage [18-20,22,23]. Those health care providers who had positive attitudes toward NASG use for the management of PPH were 1.87 times more likely than those who had poor attitudes (OR=1.87, 95% CI: 1.18- 2.56) (Figure 4c).
| Study | Clear sampling criteria | Participants and setting | Measurement ofexposure | Objective and/or question | Identification of confounding factors | Strategies to deal with confounding factors | Measurement ofoutcome | Appropriatestatistical analysis | Score |
|---|---|---|---|---|---|---|---|---|---|
| Bekele et al [18] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Merkin Bekele et al [19] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Kettema et al [20] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Yeshitila et al [21] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Taye et al [22] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Ababo Z, Woldesselese F [23] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| F. O. ADAMU-ADEDIPE [24] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| O. A., L. Y.O., O. A. and P. O.A.[25] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Kombo, Salihu A. Shehu, Sani[26] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | 6 |
| Ohaeri et al [27] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Onasoga OA et al [28] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Enuku et al [29] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | 6 |
| Aina et. al [30] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Desta et al [15] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Akingbohungbe O et al [31] | Yes | Yes | No | Yes | No | No | Yes | Yes | 5 |
| Akinyemi et al [32] | Yes | Yes | Yes | Yes | No | No | No | Yes | 5 |
| Mbaruku, G., Therrien, M.S., Tillya, R. et al [33] | Yes | Yes | No | Yes | No | No | No | Yes | 4 |
| Average | |||||||||
| Author | Year of Publication | Country | Study design | Participant | Samplesize | Utilize NASG | Prevalence of NASG utilization |
|---|---|---|---|---|---|---|---|
| Bekele et al [18] | 2020 | Ethiopia | Cross sectional | Health careproviders | 210 | 76 | 36.2 |
| Merkin Bekele et al [19] | 2023 | Ethiopia | Cross sectional | Health careproviders | 394 | 121 | 30.71 |
| Kettema et al [20] | 2023 | Ethiopia | Cross sectional | Health careproviders | 244 | 110 | 45.1 |
| Yeshitila et al [21] | 2021 | Ethiopia | Cross sectional | Health careproviders | 412 | 199 | 48.4 |
| Taye et al [22] | 2023 | Ethiopia | Cross sectional | Health careproviders | 360 | 140 | 39 |
| Ababo Z, Woldesselese F [23] | 2021 | Ethiopia | Cross sectional | Health careproviders | 377 | 148 | 39.2 |
| F. O. ADAMU-ADEDIPE [24] | 2021 | Nigeria | Cross sectional | Midwives | 101 | 31 | 30.7 |
| O. A., L. Y.O., O. A. and P. O.A.[30] | 2021 | Nigeria | Cross sectional | Midwives | 100 | 35 | 35 |
| Kombo, Salihu A.Shehu, Sani [26] | 2018 | Nigeria | Cross sectional | Health careproviders | 84 | 30 | 35 |
| Ohaeri et al [27] | 2017 | Nigeria | Cross sectional | Midwives | 177 | 25 | 14.1 |
| Onasoga OA et al [36] | 2015 | Nigeria | Cross sectional | Midwives | 112 | 52 | 46.4 |
| Enuku et al [29] | 2018 | Benin | Cross sectional | Midwives | 150 | 63 | 42 |
| Aina et. al [34] | 2020 | Nigeria | Cross sectional | Midwives | 198 | 45 | 22.7 |
| Desta et al [15] | 2020 | Ethiopia | Cross sectional | Health careproviders | 338 | 121 | 35.8 |
| Akingbohungbe O et al [31] | 2021 | Nigeria | Cross sectional | Midwives | 133 | 98 | 73.68 |
| Kassie et al [35] | 2022 | Ethiopia | Cohort | Health careproviders | 302 | 56 | 18.54 |
| Akinyemi et al [32] | 2022 | Nigeria | Mixed Method | Midwives | 164 | 89 | 54.26 |
| Mbaruku G et al [11] | 2018 | Tanzania | Cross sectional | DHS Data | 1713 | 457 | 26.68 |
A key finding of this systematic review and meta-analysis was that the use of NASG for the management of PPH among healthcare workers in sub-Saharan Africa was 37%. Although this represents moderate adoption, the rate continues to be noticeably low considering that NASG has been encouraged by the WHO for more than a decade to address high maternal mortality from PPH in low-resource settings [1,2]. Clearly, limited awareness, training opportunities, and lack of resources hindered widespread adoption, as seen elsewhere [4].
Notably, there was considerable heterogeneity among the included studies. Subgroup analysis helped reduce but did not eliminate heterogeneity. In some individual studies, small sample sizes can also affect estimates. However, a larger overall sample size for a meta-analysis produces a stronger pool of data despite heterogeneity.
Three main factors associated with NASG use were examined. Significant positive associations were reported between NASG use and health professionals’ knowledge of it, previous NASG training, and positive attitudes toward its use. This modifiable barrier allows goal implementation to further extend NASG adoption, as suggested in other studies [26,27]. Improving education on the use and benefits of NASG and providing training programs can help address knowledge and skills gaps [6,15]. Overcoming behavioral barriers by demonstrating the effectiveness of NASG may also lead to adoption [37,38].
One limitation is that the included studies were cross-sectional only, preventing causal inference. Future studies with longitudinal designs may better predict the prognostic value of findings related to NASG use. There was also a risk of publication bias, which was addressed through the use of statistical methods. However, the findings provide valuable insights to guide NASG promotion strategies in resource-limited settings with high maternal mortality from PPH.
In conclusion, the use of NASG for the management of PPH in sub-Saharan Africa remains suboptimal but has increased in recent years. Improving knowledge, training, and attitudes among providers represents a useful strategy to improve NASG uptake and reduce preventable maternal deaths due to obstetric hemorrhage throughout the region.
Acknowledgments: The authors would like to thank Wollo university for their training of systematic review and meta-analysis.
Ethics and dissemination: The systematic review and meta-analysis will not undertake any first-hand data collection and therefore do not require ethical approval.
Declaration of Conflicting Interests: The authors of this article stated that they have no potential conflicts of interest related to the research, authorship, and publication of the article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement: The data will be available with the reasonable request.
| Study | Clear sampling criteria | Participants and setting | Measurement ofexposure | Objective and/or question | Identification of confounding factors | Strategies to deal with confounding factors | Measurement ofoutcome | Appropriate statistical analysis | Score |
|---|---|---|---|---|---|---|---|---|---|
| Bekele et al [18] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Merkin Bekele et al [19] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Kettema et al [20] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Yeshitila et al [21] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Taye et al [22] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Ababo Z, Woldesselese F [23] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| F. O. ADAMU-ADEDIPE [24] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| O. A., L. Y.O., O. A. and P. O.A.[25] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Kombo, Salihu A. Shehu, Sani[26] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | 6 |
| Ohaeri et al [27] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Onasoga OA et al [28] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Enuku et al [29] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | 6 |
| Aina et. al [30] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Desta et al [15] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Akingbohungbe O et al [31] | Yes | Yes | No | Yes | No | No | Yes | Yes | 5 |
| Akinyemi et al [32] | Yes | Yes | Yes | Yes | No | No | No | Yes | 5 |
| Mbaruku, G., Therrien, M.S., Tillya, R. et al [33] | Yes | Yes | No | Yes | No | No | No | Yes | 4 |
| Study | Clear sampling criteria | Participants and setting | Measurement ofexposure | Objective and/or question | Identification of confounding factors | Strategies to deal with confounding factors | Measurement ofoutcome | Appropriate statistical analysis | Score |
|---|---|---|---|---|---|---|---|---|---|
| Bekele et al [18] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Merkin Bekele et al [19] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Kettema et al [20] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Yeshitila et al [21] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Taye et al [22] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Ababo Z, Woldesselese F [23] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| F. O. ADAMU-ADEDIPE [24] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| O. A., L. Y.O., O. A. and P. O.A.[25] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Kombo, Salihu A. Shehu, Sani[26] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | 6 |
| Ohaeri et al [27] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Onasoga OA et al [28] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Enuku et al [29] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | 6 |
| Aina et. al [30] | Yes | Yes | Yes | Yes | No | No | Yes | No | 5 |
| Desta et al [15] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 |
| Akingbohungbe O et al [31] | Yes | Yes | No | Yes | No | No | Yes | Yes | 5 |
| Akinyemi et al [32] | Yes | Yes | Yes | Yes | No | No | No | Yes | 5 |
| Mbaruku, G., Therrien, M.S., Tillya, R. et al [33] | Yes | Yes | No | Yes | No | No | No | Yes | 4 |
