ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Ophthalmology Department, Federal Teaching Hospital, Imo State, Nigeria.
2Department of Family Medicine, University of Port Harcourt Teaching Hospital, Rivers State, Nigeria.
3Department of Family Medicine, State House Hospital, Abuja, Nigeria.
Ophthalmology Department, Federal Teaching Hospital, Imo State, Nigeria.
Email: emeonyealozie@gmail.com
Received : Nov 20, 2024,
Accepted : Dec 19, 2024
Published : Dec 26, 2024,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Onyia O (2024).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Craniocerebral gunshot injuries in the past were usually described and managed in military settings; but nowadays they are increasingly being encountered in civilian and urban settings, especially in developing countries. Although less prevalent than closed head trauma, penetrating head injury carries a worse prognosis [1]. The surgical management of gunshot wounds to the head is still a challenging issue [2]. Even with the experience acquired from the two World Wars and multiple local wars, the surgical management of such patients still needs further discussion because mortality and morbidity remain high despite technological improvements in the last decades [2,3]. Advances in weapons technology and the increased accessibility of military grade firearms to civilians has changed the nature of domestic gunshot injury, thereby complicating clinical decision-making [4,5]. The largest retrospective studies to date have shown that penetrating gunshot wounds to the head are very often fatal even with appropriate medical and surgical treatment, with 71% of patients dying at the scene, 66-90% of those dying before reaching a hospital, and up to a 51% survival rate among those reaching the hospital alive [6-8]. So, management of gunshot wounds to the head from bullets, shotguns, blasts, explosions of grenades and mines have become routine experience at Neurosurgical centres in many countries with civil armed conflict [9]. In addition, management of such injuries in an emergency is a challenging task. It is basically a staged procedure which involves maintenance of the airway and circulation, control of bleeding, assessment of wound, debridement and primary repair of defect, elective management of associated soft-tissue and osseous defects, and rehabilitation of associated disability [10].
In this report, we highlight a case of gunshot injury to the face that is unique due to the peculiar trajectory of the bullet, mixed pattern of injury and damage to surrounding structures.
Our patient is a 50-year-old female who was a passenger in a moving privately-owned vehicle that was flagged to pass through a checkpoint, manned by policemen. Shortly afterwards unknown gunmen attacked the police checkpoint and fired sporadically. At the noise of gunshots, she turned and looked back while still inside the car, only to come face to face with a stray bullet. She was hit in the face and was immediately taken to a nearby hospital where she was assessed and referred. At the referral hospital, she was noted to be fully conscious, but in painful distress, and was bleeding profusely from the left eye, nose and mouth. A bullet entry point was noted on the right cheek, directly on the zygomatic bone, and about 1.5 cm anterior to the temporo-mandibular joint. The patient had difficulty opening her mouth, as a result. An exit wound was found on the medial canthal area of the left eye, and measured about 2x3 cm, appearing to align well with the entry point. Another entry point was noted about 4 cm anterior to the angle of the left jaw, and a hard mass was felt on palpation of the left cheek. There was no 2nd exit wound.
Piecing this jigsaw puzzle of findings together, the most putative mechanism of injury in this patient is that the bullet entered through the right cheek, traveled through the complex bones of the face without affecting the brain, and exited through the medial canthal area of the left eye, diametrically opposite its entry point. Upon exit, it ricocheted off the metal body of the car she was seated in, and re-entered through her left cheek, where it was lodged. This peculiar trajectory created a combination of perforating and penetrating injury, with a trail of dedestruction and permanent cavitations. The possibility of being hit by 2 stray bullets was also entertained, but was later discounted since there was only one puncture hole in the rear windshield of the car; in addition to eyewitness accounts corroborating the single bullet hit. No other occupant of the vehicle was hit. She was co-managed by the Neurosurgery, Maxillofacial and Ophthalmology teams on call.
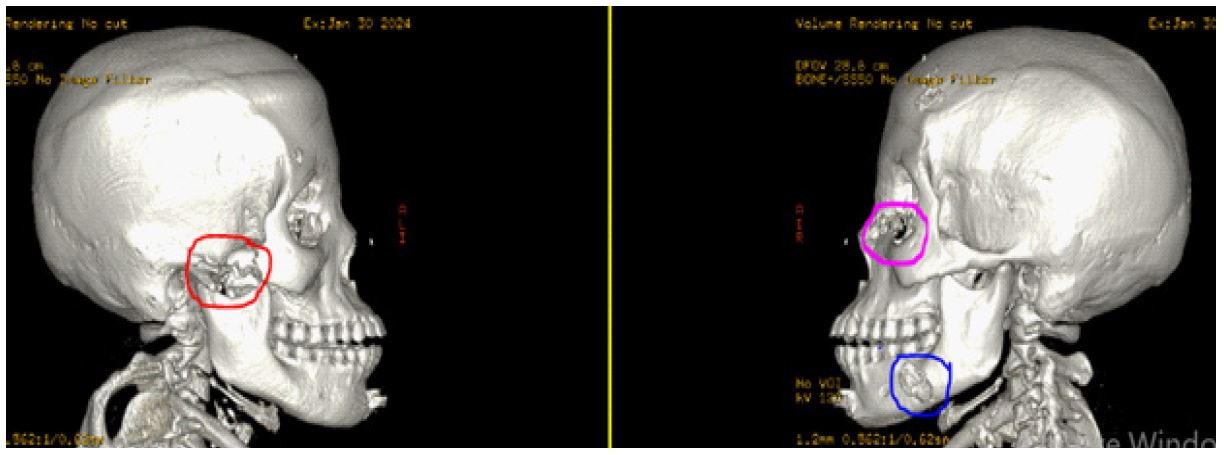
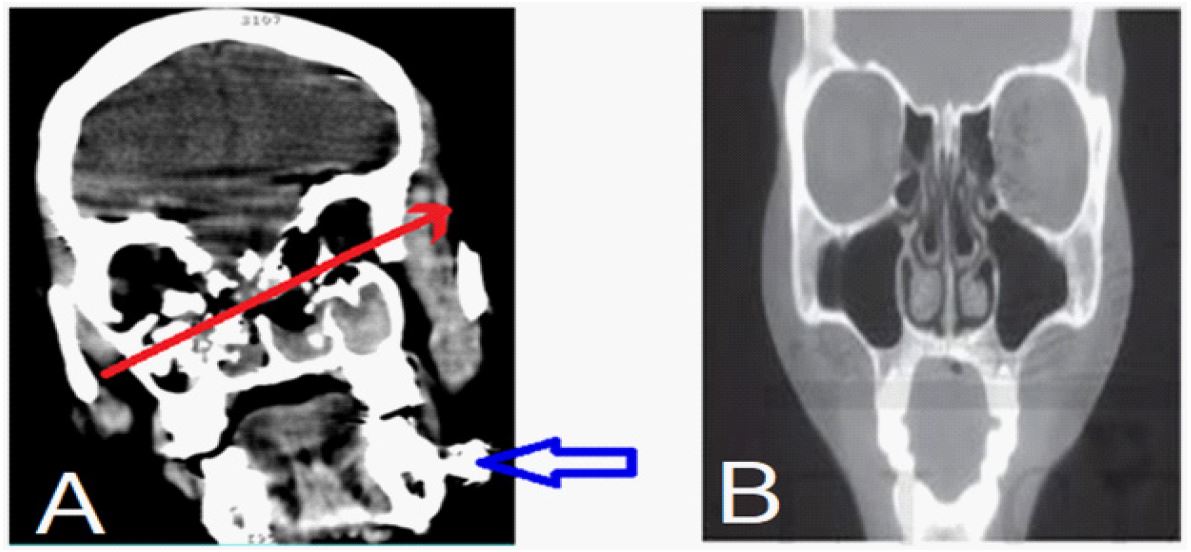
An urgent computerized tomography scan of the head with 3D reconstruction was done (Figure 1), and revealed a displaced comminuted fracture of the right zygomatic bone at the entry site (red circle), and destruction of the left orbit medial wall at the exit site (purple circle). In addition, there was also the presence of a radio-opaque material lodged in the soft tissue of the left cheek; assumed to be the bullet or its fragment (blue circle in Figure 1; blue arrow in Figure 2). There was no obvious brain tissue involvement.
The patient was managed conservatively with generous analgesia, intravenous antibiotics, intravenous fluids, tetanus toxoid, topical ocular antibiotics, and daily wound dressing. Her Glasgow coma scale at presentation was 15/15 (E-4, V-5, M-6), and remained so all through her admission. Her vital signs were also noted to be stable throughout admission, except for an iso lated temperature spike for which she was given Paracetamol. The maxillofacial unit scheduled her for soft tissue exploration of the retained foreign body in the left cheek, with possibly an open reduction and internal fixation under general anaesthesia. Later, a bullet was extracted from the swelling on the left jaw area where the second entry wound was located. There was no obvious bone tissue damage in this area.

The neurosurgery unit assessed her and did not deem it necessary for any immediate intervention since she was stable. The patient was depressed with her condition, and on several occasions, refused medical assessment and treatment. She received extensive counselling sessions, and this was very helpful in her management.
A review by the ophthalmology team noted the following key findings:
Right eye: Visual acuity of 6/60, ecchymosis and lid edema, intact eyeball, and sluggishly-reacting pupil. Fundoscopy revealed chorioretinitis sclopetaria with intra and subretinal haemorrhages at the posterior pole.
Left eye: Visual acuity of ‘No Light Perception’, ecchymosis and lid edema, mild ptosis, exit wound in the left medial canthal area, destruction of the medial wall of the left orbit, laceration and denudation of the medial part of the left eye lower lid, intact and laterally deviated eyeball, with a fixed dilated unreactive pupil. Fundoscopy revealed multiple chorioretinitis sclopetaria with intra and subretinal haemorrhages in the posterior pole and macula.
She was discharged after 12 days on admission, with significant resolution of facial swellings and improved mouth opening, as assessed by the maxillofacial unit. At one-week post-discharge follow-up visit to the eye clinic, her visual acuity remained 6/60 in the right eye, and ‘No Light Perception’ in the left eye. Posterior segment findings remained essentially same. She was psychologically upbeat and eager to know what was to be done for her vision, the limited opening of her jaw, which was affecting her feeding, difficulty with reading and recurrent upper airway infections. She was referred to a center with oculoplastic and low vision capability, advised to use protective eyewear for the only seeing eye, to eat semi-solid food as well as to attend her follow-up appointments with the maxilla-facial and Otorhinolaryngology team.
Epidemiology of gunshot injuries
Globally, in 2016, 251,000 deaths resulted from firearms injuries caused by events not related to war [11]. Recently, insecurity due to the use of firearms has become endemic and an epidemic worldwide, leading to serious injuries and deaths which affect both military and civilian populations [12-17]. Gunshot injuries account for the most homicides in the United States of America, accounting for an estimated 46 deaths every day [18]. Other studies have estimated over 90 deaths every day caused by firearm-related injuries [19]. Between 1999 and 2013, firearm-related injuries caused the death of 462,043 Americans [20]. In addition to mortality, firearm injuries also cause a massive burden on the health infrastructure, with 282,542 emergency discharges recorded in the USA between 2009 and 2012 [19].
Gunshot injuries were first reported in West Africa following the Nigerian civil war of 1967-1970 [16]. It is the second commonest cause of death per 1000 in Transkei region of South Africa [21]. In Africa, the Sahelo-Saharan belt has long been an area of instability and insecurity [16,22]; however, violence became more pronounced in the 2000s with the birth of armed jihadist groups like Boko Haram (BH), Al-Qaeda in the Islamic Maghreb (AQIM), and Movement for Oneness and Jihad in West Africa (MOUJAO), and the consequences of the Libyan revolution. [16,17,22-26] The causes of gunshot injuries in Nigeria like many other African and developing world include communal clashes, sectarian religious crises, military violence, armed robbery, hunting, political violence, students’ cultism activities and rarely sporting and suicidal attempt [27-30]. In a retrospective descriptive study of all the patients with firearm injury aged 19 years or under who presented at the emergency room of Alex Ekwueme Federal University Teaching Hospital, Abakaliki Ebonyi State, and National Orthopaedic Hospital Enugu (both in south-eastern Nigeria), over a period of 15 years (1st January 2005 to 31st December 2019), Omoke NI and Lasebikan OA, [31] noted a prevalence of 1.2 per 1000 Emergency Department attendance. The male-to-female ratio was 1.8:1, and the mean age was 13.98 ± 5.6 years. The preponderance of firearm injury was in the rural areas, during the dry season, at home, and in the daytime. Armed robbery (20, 35.7%) and communal clash (7, 12.5%) were the two topmost incidents leading to gunshot wounds. Lower extremity was the topmost anatomical region involved.
Nnadi IG and Egejuru RO, [32] in a post-mortem study in Owerri over a period of 10 years (2001-2010), noted 101 cases of gunshot injuries which constituted 20.8% of all the postmortem examinations conducted in FMC Owerri. Ninety-six per cent of the victims were males; mean age was 52.2±21.3 years and the age range was 19-71 years. The most affected age groups were those in the 21-30 age groups followed by 31-40 years. The most frequent site of entry wound was the thorax (chest), followed by the head/neck and abdomen. The highest cases of gunshot injury occurred in 2003, followed by 2009.
Gunshot injuries can be devastating especially when it involves vital organs and could result to instant death. The cost of treating patients that survive these injuries could be enormous especially when the injuries are to the head, chest, abdomen and the spine [33-35].
Ballistics concepts and the pathophysiology of gunshot injury to the head
Firearms responsible for gunshot injuries are commonly stratified by the velocity of the expelled projectile. High-velocity projectile injuries are typically from firearms with a muzzle velocity greater than 2000 ft/s (like the AK-47), and are associated with more substantial tissue damage [36]. Low-velocity projectile injuries are caused by firearms with muzzle velocities less than 2,000 ft/s (commonly pistol calibers) [36]. Shotguns are a common example of a low-velocity firearm (1,000-1,500 ft/s), but they provide a unique ballistics pattern that differs from the behavior of a single projectile [37,13,38,39]. The most commonly used weapon in Africa’s conflict zones is the Kalashnikov and its derivatives [40].
The ability of any penetrating object to penetrate the skull and cause primary brain injury is dependent on the ballistic properties i.e. kinetic energy, mass of projectile, velocity, shape, angle of approach, the characteristics of intervening tissues, etc and any secondary projectiles formation such as fragments of bone or metals [1,41]. The efficiency of energy transfer is dependent on multiple factors including the trajectory stability, distance travel, entrance profile of the projectile, and the amount of yaw (the angle of deviation from the projectile’s long-axis) [39,42]. The caliber and material of the bullet, the tissue type impacted, mechanism of tissue disruption, and trajectory within the body, also contribute to the projectile’s energy transfer [39,42].
The kinetic or wounding energy is defined by the relationship: E = 1/2MV2. Velocity can be represented as E= 1/2 M (Vi2 - Vr2), where M is the mass of the projectile, Vi is the impact velocity and Vr is the residual velocity in the case of perforating wound [43,44]. This implies velocity of the projectile has a greater influence than the mass alone, meaning that the bullet of an AK-47 assault rifle, which weighs 7.9 g and has an initial velocity of 720 m/s, has a kinetic energy of 2635 ft/lb (1.77 m/g). Projectile velocity from firearms in handguns is less than that of rifles, varying usually from 180 m/s to 450 m/s. When the velocity exceeds 700 m/s, the wounding capacity of the projectile is significantly increased, leading to more severe brain damage, more bone fragmentation of calvarium, and associated enhanced secondary brain cavitations [45,46]. However, a bullet does not need to penetrate the skull to cause intracranial damage; the mechanism of injury in these are either a blunt force or secondary bone fragments [47]. The velocity of the missile is also important in tangential wounds, having the ability to release sufficient energy to cause intracranial damage without skull bone damage [48]. A projectile, while travelling through the air loses kinetic energy rapidly due to resistance [49], which causes reduction in projectile velocity which also depends on the shape of the projectile. Bullets can be blunt-nosed, fully or half jacketed and hollow tipped to increase deformity, to ensure more damage to target. The sharper the nose of a bullet, the lesser the decrease in velocity due to air resistance [50]. Our patient was most likely shot with an AK-47 rifle, which is a common rifle used in most conflicts in this region of the world.
The Neuro-ophthalmic cost of a stray bullet
Based on the outcomes of a prospective study, all patients with gunshot wound to the head should initially receive aggressive resuscitation [50]. Also, in a 5-year retrospective review of 132 civilian patients with craniocerebral gunshot wounds, increasing survival was associated with aggressive resuscitation in all patients, and resuscitation with blood products and hyperosmolar fluids were independently associated with survival [7]. Patients with a Glasgow Coma Score > 8, normal pupil reaction, and single-lobe brain injury may benefit from early aggressive management [51]. Our patient received aggressive management in the accident and emergency department, despite having a stable Glasgow Coma Score and vital signs.
Neurosurgeons all over the world agree that patients with brain injury should have a head CT scan as soon as they arrive at the hospital. Plain radiographs of the head can be helpful in assessing the bullet trajectory, the presence of large foreign bodies, and the presence of intracranial air. However, when CT scanning is available, plain radiographs are not essential and are not recommended as routine [52]. No imaging technique is faster and more accurate than CT. It has almost no contraindications, except for pregnant women. A CT scan of the head defines the bullet’s trajectory, entry and exit sites, extent of intracranial fragments and proximity to major blood vessels and the ventricles, and pressure on the ambient cistern. In addition, a CT scan of the head will determine the need for surgery and define the strategy for surgical treatment. It is the recommended imaging modality with 5-mm-thick continuous slices along the Reid line from the vertex to the foramen magnum for evaluating cranial trauma [53]. The role of cranial CT in our patient cannot be over emphasized as it illuminated the bullet trajectory and the destruction it left in its trail. Fortunately, the bullet missed the brain. Therefore, the CT formed the cornerstone of the decision to adopt a conservative management by the neurosurgery team, since there was no radiological evidence of brain injury.
Craniofacial region is the most favorite target for gunshot injuries, most of the times especially in close range firings. The reason is that head and neck region is most complex structure in the human body which contains important contents, i.e. brain, upper portion of the spinal cord, eye, nose, oral cavity, rich vascular network due to the great vessels; damage to it results in high incidence of morbidity and mortality [54]. Found that out of 178 gunshot wounds to the face, 40% involved the frontal bone and cranium, 9% involved the orbits, 14% involved the lower midface (maxilla), 13% involved the mandible and 24% involved multiple sites [55]. Gunshot wounds to the midface results in high prevalence of facial fracture (35%), globe injury (20%), vascular injury (20%) and intracranial penetration (20%) [56].
Complications associated with facial injuries include periorbital cellulitis, diplopia, loss of vision, facial nerve paresis or paralysis, cerebrospinal fluid leak, soft tissue loss, bony malunion, malocclusion, trismus, oro-antral fistula, nasal obstruction or stenosis, and choanal stenosis [57]. In their study reported 4,139 patients with gunshot wounds over 4 year period; 6% (247) had injuries to the face. 38% of these had isolated wounds to the face, whereas the remaining 62% had associated injuries to other body areas. Thirty six patients (15%) died following admission. All the deaths were secondary to injuries to the chest, abdomen or brain. There were no deaths associated with isolated facial injuries [58]. Our patient had isolated facial injuries and was fortunate to survive. A study by [59] showed a profound male preponderance of 95.5%, and the most common complication reported was loss of vision. Our patient lost vision in her left eye, and had severe degradation of vision in the right eye. Both eyeballs were essentially intact. The major cause of visual morbidity in our patient was attributed to chorioretinitis sclopetaria.
A closed globe (ocular) injury from the forces of a high velocity object (projectile) passing very close to the globe can cause chorioretinitis sclopetaria. Chorioretinitis sclopetaria is the rupture of the choroid and retina. Deformation from the sudden strike causes the chorioretinal layers to “split and retract” leaving the intact sclera bare [60]. The location of the rupture determines visual recovery and final best-corrected visual acuity (BCVA) [61]. There is no open globe injury, and intraocular pressure is maintained. The indirect and direct shock-wave forces cause chorioretinal rupture, vitreous hemorrhage, and later, white fibroglial proliferation [61]. In 1974, first reported histopathology of chorioretinitis sclopetaria in a postmortem exam of a gentleman that was shot in the eye [62]. Sclopetaria pathology was described as macular defects of Bruch’s membrane and choroid with extensive photoreceptor loss and hyperplasia of the retinal pigment epithelium. Loose fibrous tissue replaced the ruptured choroid and retina, and is later replaced with dense connective tissue resulting in scarring [60]. Blunt ocular trauma to a closed globe can manifest into various injuries to the posterior segment. Chorioretinitis Sclopetaria is a coup injury which means it is damage at the site of impact. The projectile injury results in an absent retina and choroid in the same quadrant as the injury. Conversely, contrecoup injury is damage to tissue at the opposite site of impact which can result in commotio retinae, choroidal rupture, etc [63,64].
The clinical and pathological findings are a result of differences in elasticity in the various parts of the eye. Bruch’s membrane is inelastic and ruptures easily with compressive forces. The choriocapillaris is attached to this membrane which further leads to acute subretinal hemorrhage. Retinal Pigment Epithelium is also inelastic, making rupture also more likely. Retina and Sclera are elastic, thus very high impact energy, usually through high velocity projectile objects like a bullet, is necessary to cause disruption and damage. The result is a full-thickness defect involving the choroid, Bruch’s membrane, retina, with an intact sclera. As the etiology of sclopetaria is due to a high velocity object passing near the globe, it can create significant shock waves with enough force to retract the choroid and retina with bare sclera at the site of injury [65]. In the weeks following the injury, a dense fibrous tissue forms between the choroid and retina with scar formation with claw-like irregular borders. The diagnosis of Chorioretinitis Sclopetaria is clinical with dilated fundus findings showing retinal hemorrhages, bare sclera, vitreous hemorrhage, intra-retinal or subretinal hemorrhage along with sequelae from comorbidities [66].
Diagnostic imaging can yield supporting evidence for diagnosis. The physical exam findings on the dilated fundus exam can reveal subretinal hemorrhages, vitreous hemorrhage, bare sclera, macular edema, choroidal breaks, and disc edema [66]. Follow-ups after initial assessment can show fibrous tissue which develops after blood at the site of injury is reabsorbed [63]. It was previously assumed that the secondary fibrosis and scar formation between the choroid and RPE post-rupture would prevent retinal detachment. However, recent studies in 2014 by Papakostas et al. noted retinal detachment in three cases of sclopetaria with extensive orbital injury and intra-orbital surgery. Therefore, dilated fundus examination in the weeks following injury should be done to monitor for development of a retinal tear or detachment [67].
There is no consensus on the management of chorioretinitis sclopetaria due to the low number of reported cases as well as the variability in injury. A case-by-case approach is indicated in blunt ocular trauma, and treatment teams need to be cognizant of chorioretinitis sclopetaria along with possible comorbidities including orbital floor fracture, commotio retinae, retinal detachment, and intraorbital foreign body/ies. Often, in the absence of other indications for surgery, patients may be carefully observed as the retinal ruptures heal themselves due to the large degree of glial proliferation at the site of the injury.
The majority of treatment for sclopetaria tend to follow two paths of management; Surgery versus Observation. The treatment depends on each individual scenario. If there is concern for globe rupture and/or retinal detachment alongside sclopetaria, surgery is indicated. Immediate surgical intervention may not benefit the final visual recovery, however the sample size for such interventions are currently low. Immediate surgical intervention includes foreign body removal, globe exploration, pars plana vitrectomy, scleral buckle, enucleation, etc., and resulted in final Best Corrected Visual Acuity (BCVA) worse than 20/20 more significantly than patients with observation (91.7% vs 78.4%). Delayed surgery was performed less often but resulted in 77.8% of the patients (7/9) with BCVA worse than 20/20 [61].
Patients with with sclopetaria are at increased risk of progression or delayed presentation of vitreous hemorrhage and retinal detachment. Retinal detachment is considered less likely due to the fibroglial scarring between the choroid and retina, as well as the typically young patient population with intact vitreous. However, occurrence is possible with severe repercussions to a missed diagnosis [61,68].
Prognosis of chorioretinitis sclopetaria depends on type of injury, object of injury, location of primary penetration and location of rupture. Most patients experience improvement in final best corrected visual acuity from time of injury, but only 16.4% achieve 20/20 vision [61,65].
Visual Prognosis based on study [61]:
Lower muzzle energy (air-gun pellet and paintball) resulted in poorer visual outcome compared to higher muzzle energy (bullet and BB).
Temporal and macular sclopetaria had poorer visual acuity and were less likely to achieve 20/20 vision (our patient had temporal and macular sclopetaria).
Macular hole or maculopathy increased the risk of incomplete visual recovery.
Eyelid lacerations were found to have poorer visual prognosis possibly due to more profound ocular injuries (our patient had left lower eyelid laceration).
Optic nerve avulsions had poor visual outcomes.
In addition, our patient required oculoplastic reconstruction of the defect in the medial canthal area of the left eye. She was was referred to a peripheral centre with oculo-plastic capability.
Key messages
1. It is possible to have this type of gunshot injury with two penetration points by a singular projectile.
2. Gunshot injuries to the face can lead to psychosocial problems in victims, often requiring a multidisciplinary long-term management approach.
3. Insecurity and gun violence continue to show an upward trend, with incursions in civilian and urban settings. Advocacy to introduce or strengthen gun control legislations will help stem the tide of gunshot injuries.
4. Community sensitization with information, communications and educative materials on best response tactics to active shooter scenarios is important in dire insecure areas.
Gunshot injury to the craniofacial region results in both functional deficits and aesthetic blemish; which in turn can lead to psycho-social problems. Cosmetic and plastic reconstruction, as well as the rehabilitation of the associated deformities, is quite a challenging task. Insecurity seems to continue on an upward trajectory endangering the lives and well-being of innocent citizens. Governments should step up to the responsibility of protecting the lives and properties of their citizenry.
