ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Center for Infectious Diseases, The Second Affiliated Hospital of Air Force Medical University, China.
Center for Infectious Diseases, The Second Affiliated Hospital of Air Force Medical University, China.
Tel: +86 29 84777853; Fax: +86 29 83537377;
Email: jiangh518@126.com
Received : Jan 19, 2025,
Accepted : Feb 17, 2025
Published : Feb 24, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Jjiang H (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Ascites is a common condition in cirrhotic liver disease that may affect up to 50% of compensated liver disease patients [1]. Infection of the ascitic fluid is a serious complication associated with a substantial increase in the risk of mortality [2]. Timely diagnosis and adequate anti-infective treatment are crucial. Although E. faecalis and E. faecium among Enterococcus kindred account for more than 90% of infections, E. avium has been increasingly documented as a causative agent in human infections [3-7].
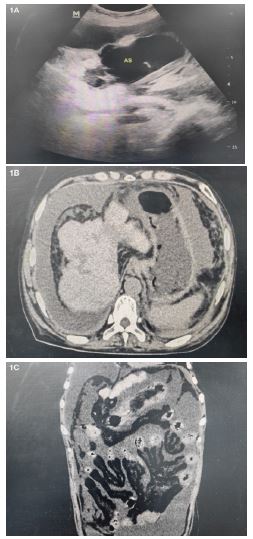
We present a 50-year-old woman hospitalized on November 9, 2023 with general abdominal pain worsened progressively of 9 days’ duration and ceftazidime was inefficacy. The patient’s medical history includes a six-year duration of autoimmune hepatitis with hepatocirrhosis, for which she has been regularly prescribed ursodeoxycholic acid capsules at a dosage of 250 mg three times daily. No history of glucocorticoid use and abdominal surgery. On admission, the patient presented with diffuse abdominal pain and weakness. The physical examination revealed afebrile status, blood pressure of 103/64 mmHg, pulse rate of 93 beats per minute, as well as diffuse abdominal rebound tenderness. No peripheral stigmata of infective endocarditis. B-ultrasonography showed a large amount of ascites, with floating objects presented in large grids (Figure 1a). Abdominal Computed Tomography (CT) studies demonstrated the peritoneum was thickened, the adipose space in the abdominal cavity was blurred, and the subcutaneous adipose layer on both abdominal walls was cloudy (Figure 1b & Figure 1c). The relevant laboratory data on admission were as follows: white blood cell 28.34E+09/L; neutrophil 26.56E+09/L; c-reactive protein 83.69 mg/dl; procalcitonin 11.59 ng/mL; lactic acid 7.41 mmo/L. The analysis revealed a leukocyte count of 3900E+06/μL with 80% neutrophils in the turbid abdominal effluent. The empirical therapy is initiated with meropenem (1g i.v. 8 hrly). The presence of E. avium was rapidly detected within 1 day using NGS. At once, linezolid was added to the meropenem anti-infection treatment regimen. It took 6 days for E. avium to be identified through culture-based methods. Antibiotic therapy consisting of meropenem (1g i.v. every 8 hours) and linezolid continued for 5 weeks, in conjunction with peritoneal lavage. The patient’s abdominal pain was alleviated, accompanied by a significant improvement in the clarity of the effluent. Then, the patient experienced an uneventful recovery and was discharged on day 36. Since her discharge from the hospital, she has been residing in her residence and remains ambulatory with crutches until February 1, 2024. (We have received written informed consent from the patient for publication of case details. We depersonalized data to disable the identification of the patient).
The abdominal infection are critical conditions that necessitate prompt diagnosis and treatment. NGS Assist timely diagnosis of the responsible microorganism and adequate anti-infective treatment. In this case, the patient benefited from earlier (5 days) and more targeted antimicrobial therapy facilitated by NGS methods, potentially reducing the substantial morbidity and mortality associated with the infections. When we get the result of NGS in this case, we repeatedly interrogated the patient’s epidemiological history. The patient had utilized chicken manure fertilization in the field. Initially classified under the Streptococcus genus as S. avium (due to its frequent isolation from chicken feces). It is likely that infection occurs primarily through the fecal-oral route. The patient had definite fever, nausea, vomiting, and diarrhea before the onset of the disease, which is consistent with previous E. avium reports. The patient’s lack of response to ceftazidime treatment before admission may be interpreted as natural resistance of Enterococcus to cephalosporins. The result of NGS was proved as abdominal fluid the classical blood culture test showed the same bacterial.
Disclosure: The authors declare that they have no competing interests.
Patient consent: Informed consent was obtained from the patient included in this brief report.
Author contribution: Shiqi Chai, Wenzhen Kang, Yi Gang, Hong Jiang jointly participated in the treatment of the patient. Shiqi Chai wrote the manuscript. Wenzhen Kang, Yi Gang, Hong Jiang revised the article.
