ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*School of Nursing and Midwifery Umma University, Kajiado, Kenya.
School of Nursing and Midwifery Umma University, Kajiado, Kenya.
Email: grenyomuira@yahoo.com
Received : Jan 14, 2025,
Accepted : Feb 20, 2025
Published : Feb 27, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Wainaina GM (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
The health status of mothers and children is an indicator of a country’s well-being. This is because, women and children form a large percentage of every population and their health shows health improvements in every community. Unfortunately, women and children die each day due to preventable factors that have been identified but not dealt with fully.
In 2014, the global maternal deaths were estimated to be 289 000 with the sub-Saharan Africa region accounting for 62% (179 000) deaths followed by Southern Asia at 24% (69 000) [1]. But by 2020, there was only a slight improvement-down to an estimated 287,000. In terms of reaching the SDGs, the 2020 Maternal Mortality Ratio (MMR) is still estimated at 223 maternal deaths per 100,000 live births.
Unfortunately, the Global Health Observatory Data (2015) presented a global maternal mortality data of 303, 000 and 546 deaths per 100,000 in sub-Sahara region indicating a worse of global situation rather than an improvement.
In Kenya, maternal mortality rate is still a problem with very slight improvements over the years. Sadly, Kenya was among 10 countries that comprised 58% of global maternal death in 2013 contributing 2% of the world deaths [2] and still is among 18 top countries with high MMR of 362/100,000. Kenya is a member of the Sustainable Development Goal, and was to reduce the maternal mortality by 75% towards the end of 2015. Unfortunately, Kenya fell short of achieving its goal. Similarly, Kenya also fell short of the Skilled Births Attendants at 62% way below the target of 90% by 2015.
It is for this reasons that the Kenyan Government has been active in championing the most recent Strategic Framework of beyond Zero to facilitate prenatal and postnatal medical treatment to women and children in Kenya towards saving lives of both mother and baby. The strategic framework focuses on five key areas: Accelerating HIV programs, influencing investment in high impact activities to promote maternal and child health and HIV control, mobilizing men as clients, partners and agents of change, involving communities to address barriers to accessing HIV, maternal and child health services and providing leadership, accountability and recognition to accelerate the attainment of HIV, maternal and child health targets [3]. All these were geared towards attaining safe motherhood which unfortunately has not been fully met.
Therefore, the researcher hopes to combine the strategy of mobilizing men as clients and agents of change, as well as involving communities to address barriers to accessing maternal and neonatal health, by giving them information about safe motherhood in order to improve maternal and neonatal health. This is in line with policy brief of 46 (2015) that suggests that the problem of maternal mortality can be curbed by implementation of knowledge delivery and technology usage. It is for this reason that this project intends to embrace technology usage and enhance knowledge distribution among the women’s men partners and other selected household members to enhance safe motherhood in order to achieve Kenyan’s vision 2030 at household and community level.
Among the many ministries that Kenya has, telecommunication has shown remarkable growth. The Communication Authority of Kenya reported that Kenya had the second highest growth rate in Africa on Telecommunication [4]. In 2019, 104% mobile phone penetration was noted [5].
However, even with mobile telecommunication spreading quickly, it is not always spreading equally [6]. Gender gaps exist especially in low and middle level countries. Women and Mobile, [6] revealed a gender gap of 21% women less likely to own a phone than their male counterparts. In 2018, GSMA noted an improvement of women owning a phone but still were 10% less likely to own a phone. That translated to 184 million fewer women owning a phone. Notably, women have always faced more challenges in terms of technological issues especially for transformational services like internet mobile technology, mobile technology in health or mobile technology in finances especially in Asia and Africa than men [6-8].
Since the policy brief of 46 (2015) suggested that the problem of maternal mortality can be curbed by implementation of knowledge delivery and technology usage, the technology gap among the women should be addressed. Women should be encouraged to access mobile technology and utilize it as well as their male partners and community and family members in order to enhance safe motherhood. Since women are the main custodians towards maternal and child health, their utilization of technology to access knowledge during the pregnancy, labor and delivery and post-partum period should be encouraged. These women include the pregnant woman, their sisters, their grandmothers as well as their mothers in law who frequently overshadows the role of men in maternal health decisions in some societies [9]. The significant men too should be involved preferably the husband of the pregnant woman since in the African context men have been noted to influence the behavior and actions of their wives [10].
It is for these reasons that this proposal suggests the embrace of mobile technology among the women (pregnant woman, mother-in-law, sister, grandmother) their partners (husband, male companion) and communities (gate keepers) to dispatch maternal and neonatal knowledge for the betterment of improving maternal and neonatal health so as to contribute to the attainment of vision 2030 and the proposed Sustainable Development Goals in Kenya and in the sub-Saharan regions. To meet this goal, the researcher hopes to describe the baseline safe motherhood information the pregnant mothers have at the beginning of the study and provide additional information to them via the short messages service through their mobile phones throughout the pregnancy period as well as to their relevant family members and assess the importance of that additional information through their phones throughout pregnancy for enhancement of maternal and neonatal continuum in Kajiado Central.
Problem statement
Maternal mortality is defined as Pregnancy related Deaths. Pregnancy-related death defines the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death. In Kenya, 32,021 women of reproductive age were reported to have died out of which 6,632 died of pregnancy related causes. Out of the 47 Kenyan administrative counties, 15 counties account for 98.7% of the total maternal deaths in the country [11].
Notably Kajiado had mortality rate of 500/100,000 as compared to the national rate of 488/100,000 against an expected national goal of 147/100,000(MDG 2015) and 70/100,000 Sustainable Development Goal, vision 2030. For a long time, many initiatives have been suggested and implemented in Kajiado county in order to improve maternal and child health care. One such initiative was the African Medical and Research Foundation (Amref) baseline survey that was done in 1994 to provide a baseline data and information in order to strengthen maternal and child health practices in Kajiado county. Findings indicated high numbers of mothers getting babies “too early” thus increasing their rates of morbidity and mortality, 80% of deliveries occurring at home and done by none skilled persons for examples relatives and neighbors.
In 2013, another initiative known as Mama na Mtoto was started in order to facilitate the attainment of the millennium development goals 4 and 5. The project aimed at reaching 200,000 women and children in order to strengthen mother and child health care [12].
Later, Amref created the “Boma” model that recognized the Maasai homestead in enhancing Maternal, Neonatal and Child Health services (MNCH). The Model revealed an Antenatal care utilization coverage of 32% in 2010 and 59% in 2012 (The Boma 2013) against a national target of 80% utilization [13]. The report also suggested a low skilled birth attendance of 24% by 2012 (The Boma 2013) against the national average of 61% [13]. A low facility delivery of approximately 5% was recorded against a 44% of national coverage [14].
Later, another initiative was commenced known as the “Helping 350 Maasai women deliver safely in Kenya” initiative. This initiative was commenced from household to community to health facility in order to create demand for service through negotiating with households as partners in healthcare. Through the One Moran Can (OMC) initiative, opinion leaders in the community, traditional birth attendants and community health workers were engaged as partners to facilitate 350 women access antenatal, labor and delivery services and postnatal services throughout the year. This enhanced accessibility of 85% coverage [14].
Other national initiatives (like the six pillars of Kenya’s Maternal and Neonatal and Child Health (MNCH) programme, was the strategic framework of the engagement of the first lady towards improvement of MNCH health, the free maternity care initiative, have all been implemented in Kajiado but unfortunately the county still ranks among the country with the highest maternal morbidity and mortality (UNFPA, KENYA 2014) against the Sustainable development goals call to reduce the maternal mortality to less than 70 deaths per 100,000 live births (United Nations 2015).
It is for these reasons that the researcher who is a nurse with a specialty of Maternal and Neonatal Health saw the need to conduct the study by involving very specific people attached to the pregnant woman and using mobile phone services to dispatch safe mother hood information throughout pregnancy. The researcher works in Umma University that is located in Kajiado County. Umma University offers nursing training and frequently involves the nursing students in both clinical and community activities in Kajiado county. The university hopes to contribute to the counties betterment in various sectors and remain relevant to the people of Kajiado County. Therefore, the researcher in conjunction with Umma university saw the need to be relevant to the members of the Community by solving part of their maternal health related challenges. The proposal therefore hopes to dispatch quality MNCH informational knowledge via mobile phones to pregnant women and the significant women and men around them. These key people will be called gatekeepers, whose mobile phone utilization towards MNCH knowledge services, hopes to enhance maternal and neonatal health in Kajiado county throughout pregnancy period.
Justification of the study
This proposal is timely because the third Sustainable Development Goal (SDG) advocates for good health and well-being by 2030 by reducing maternal mortality to 70 deaths per 100,000. Kenya is a signatory to enhance the achievement of the SDG by having their own plan of vision 2030. The proposal towards integration of family in health by using mobile phone should be a collective responsibility from the household level which falls under community level one and forms the basis of seeking good and quality health care. The proposal should be embraced and enhanced on Maternal and Neonatal Health care in Kajiado county to facilitate the accessibility and utilization of the maternal health care and achieve the vision 2030 and SDG targets.
Significance of the study
The involvement of the first level of health system at the household in the community is an investment of both knowledge and financial benefits. The upfront investment of knowledge and information to the household might help in future costly health implications of both the household and the community and the health facility and country status. The continuous involvement of the women in their continuum of care pathway in MNCH can enhance proper health and relate to better outcomes and avoid mortality and morbidities of the mothers thus increase the chances of children survival as healthy mothers are more likely to raise healthy children. Since the study proposes the incorporation of the mobile technology, this can enhance standardization of safe motherhood information in the household especially to the woman’s gatekeeper and facilitate prompt and well-coordinated response to the care towards a successful continuum of MNCH care pathway.
Research questions
1. What baseline information on safe motherhood durduring pregnancy do the pregnant mothers have in Central Kajiado County?
2. What safe motherhood information did the pregnant mother and her gatekeepers acknowledge to have acquired via their mobile phones during the mother’s pregnant period in Central Kajiado county?
3. What is the relationship between the safe motherhood information acknowledged to have been acquired via mobile phone by the pregnant mother and her gatekeepers and the implementation of the information throughout pregnancy in Central Kajiado County?
Research objectives
1. To describe the baseline information on safe motherhood that the pregnant mothers have in Central Kajiado County.
2. To highlight the safe motherhood information that the pregnant mother and her gatekeepers acknowledged to have acquired via their mobile phones during the mother’s pregnant period in Central Kajiado County.
3. To determine the relationship between the safe motherhood information acknowledged to have been acquired via mobile phone by pregnant mother and her gatekeepers and the implementation of the information throughout pregnancy in Central Kajiado County.
Maternal and neonatal health care overview
Maternal Neonatal and Child Health Care was mentioned as a rally call to reduce half a million maternal deaths, 4 million neonatal deaths and 6 million child deaths by advocating for care during adolescence, pregnancy, childbirth, postnatal period and childhood periods to be implemented between the household, communities, outpatient, outreach services and clinical settings [15]. This rally call proposed 8 packages to promote health for mothers, babies and children. These packages included: Three (3) packages of reproductive health, obstetric care and care of sick newborn and children, four (4) outpatient and outreach services packages that include antenatal care, postnatal care and child health services. Finally, was the one (1) package for integration of family and community care throughout the Maternal Neonatal and Child health (MNCH) life cycle [15]. The package that suggests the integration of family and community care throughout the (MNCH) life cycle is what this proposal hopes to highlight. The researcher hopes to highlight the need to involve the family (pregnant mother’s gatekeepers) by dispatching safe motherhood information via short messages services of the mobile phone in order to promote good MNCH.
The suggestion to adapt and implement the concept of Maternal Neonatal and child Health care was based on the idea that care should start from preconception, to pregnancy time, to birthing time and later to early postnatal time. This was highly recommended for the Sub Saharan region [16]. This concept projected financial benefits for every life saved and its implementation proposed increased maternal and neonatal coverage by 2025 inoder to reduce both maternal and neonatal dealths. The concept of Maternal Neonatal and Child Health care was based on an assumption that the health and well-being of the women, newborn and children should be closely linked and managed in a unifed way. It is therefore for these reasons that the involvement of family and community towards the health of the mother and the child is of great importance.
Notably, the need to improve maternal and neonatal and child health by involving the family and community is supported by the 4th article of declaration that states that “people have the right and duty to participate individually and collectively in the planning and the implementation of their health care”. Likewise, the seventh article of declaration states that “primary health care requires and promotes maximum community and individual self- reliance and participation in the planning, organization, operation and control of primary health care [17]. Therefore, the woman in her reproductive age needs to be conscious of herself in planning, organizing and implementation of good health as well as her family, and her community. Therefore, the inclusion of mobile technology usage to the household members seems to be a timely innovation in order to hopefully empower the reproductive age woman and her gate keepers in order to make sound decisions at the household and community level to achieve positive outcomes of reducing morbidities and mortalities.
Maternal neonatal and child health package
Maternal Neonatal and Child Health (MNCH) continuum of care pathway is an interconnection of ideas and concepts along the segments and each segments has dependence on the next or the previous one. Mothupi [18] recommends that the continuum of care in MNCH should be highly recommended and implemented by the Low- and middle-income countries. The required information that should be passed to the mother and her relevant gate keepers include information during pregnancy, labor and delivery and early post natal period. During pregnancy, there are two identified and acceptable models namely the World Health Organization Antenatal Model (WHO ANC Model) and the Focused Antenatal Care Model (FANC). The WHO ANC Model by the Focused Antenatal Care Model (FANC) highlights 4 visit. The visits can be organized as follows: First visit during 8-12 weeks, second visit during 24-26 weeks, third visit during 32 weeks and the fourth visit at 36-38 weeks. However, these dates and timing can always change so long as the woman achieves the antenatal objectives.
During the first visit, services offered include: Confirmation of the pregnancy, indicating the Expected date of delivery, documentation of the psychosocial, medical and obstetric history, classify the woman for the 4 basic ANC visits, screen for syphilis, Human Immuno deficiency Virus (HIV), proteinuria, blood group and rhesus factor, bacteriuria. Treat for syphilis and give Antiretroviral drugs if client is eligible. For preventive measures, tetanus toxoid injection is given and iron and folate tablets offered. Health education and advice and counseling include information on self-care for example hygiene, avoidance to alcohol and tobacco use, quality and quantity nutrition, safe sex, importance of rest, sleeping under an Insecticide Treated Net (ITN) and giving information on birth and obstetric emergency plan (danger signs).
Second visit services include: the assessment of both the mother and fetal well-being, by checking the vital signs (blood pressure, temperature, respirations, heart rate, oxygen saturation) of the mother and the fetal heart rate, assess significant symptoms, check record for previous complications and treatments during pregnancy. Examine for anaemia, blood pressure, fetal growth and movements as well as screening for bacteriuria and treating for helminthes, bacteriuria and HIV if eligible. Preventive measures include administration of tetanus toxoid vacvaccination, offering iron and folate tablets, offering ARVs where eligible and insecticide treated nets or offering intermitted prevention treatment for malaria during pregnancy. Review and modification of the birth and emergency plan is also reevaluated.
The third visit services include: assessing significant symptoms, checking records for previous complications and treating the current complications during pregnancy. Assess the fetal growth, screening and treatments of bacteriuria and ARV administration where applicable. Prevention of malaria and its treatment, iron and folate administration and health education on birth and emergency preparedness, infant feeding advice, postnatal care, pregnancy spacing and reinforcement on previous advice.
The fourth visit comprises of the assessment of the mother and the fetus, reexamine for anaemia, blood pressure, multiple pregnancy and malpresentation. Screening and testing for bacteriuria, ARV treatment where applicable, administration of iron and folate for preventive measures and including health education advice and counseling on birth and emergency plan, infant feeding, post natal care, pregnancy spacing and reinforcement of previous advice.
The facilitation of high-quality antenatal care can reduce maternal and newborn mortality especially if the women have contact with well-functioning and effective health system to facilitate timely prevention, detection and treatment of complications [19]. The antenatal progress is globally monitored by evaluating the first antenatal visit that mostly accounts for 90% and the fourth visit that accounts for 57% [20]. The dropout rates between the first and the fourth antenatal visit has been at times blamed for the poor uptake and implementation of safe motherhood during pregnancy period. Notably, integration of mobile technology through the Short Message Services (SMS) into antenatal coverage has shown positive effects for the uptake of the FANC visits in low- and middle-income countries to reduce the effects of the drop-outs rates [21]. This is because the SMS function has previously been to facilitate reminders to the women for clinic attendance, create an avenue for feedback, boosted self-efficacy, social support and encourage peer to peer network [21].
Since, this proposal suggests the embrace of family and the community that is around the woman of reproductive age as she goes through pregnancy, mobile technology incorporation to the family and community in order to support the woman will be the main concern. Specific content of information during pregnancy (FANC package), will be shared through the SMS platform to the pregnant woman as well as her gatekeepers in order to enhance maximum utilization and benefit acquisition of antenatal care coverage as well as contribute to the whole MNCH Continuum of care.
Success stories of mobile health coverage
In Kenya, the mobile penetration is at 109% with 96% of the Kenyan population covered by a mobile network [5]. The Audience Scapes (2014) also noted that in Kenya, 55% of women own phones verses 67% of men who own phones. The survey revealed that men were more likely (92%) to use mobile phones than women (86%). Notably, the use of Short Messages Service (SMS) ranked highest in the usage of phones than voice utilization [5]. Mobile technology has made great advancement in health, finances and other sectors. Mobile phones are very important in low and middle level countries to facilitate mobile health technology.
Mobile Health is the use of mobile telecommunication technology for the delivery of health care in support of wellness [22].
Some success stories in mobile health include positive impact among Pakistani girls on dispatch of SMS information on nutrition, health and religion (GSMA 2012). The GSMA (2012) also noted that in Afghanistan, Roshan as a major mobile service subscriber promoted culturally appropriate promotions for women th at emphasized on family and security among the Aali mothers. In Kenya, the Kenyan Ministry of Public Health and Sanitation and USAID-funded APHIA plus KAMILI developed a pilot project to help pregnant women seek antenatal care and delivery services using their mobile phones. The organization would send Short Messages Service (SMS) to remind the pregnant women of the dates of their clinics. This led to majority of women attending 4 clinics and receiving at least 2 doses of intermittent preventive treatment of malaria in pregnancy using Sulfadoxine –Pyrimethamine.
Mobile Alliance for Maternal Action (MAMA) facilitated mothers to use technology to improve health and nutrition outcomes among pregnant women and new mothers and their infants in resource-poor settings by delivering vital and culturally sensitive health messages to new and expectant mothers via their mobile phones. An analysis on the policy noted very timely maternal and newborn health messages that were culturally sensitive and gained popularity in 250 organizations in 60 countries around the world in Bangladesh and South Africa and reached over 376,000 mothers and families [12].
In addition, the Ananya Program was a multi-platform Approach to reduce maternal and infant mortality in Bihar, India. The program aimed to reduce maternal, newborn and child mortality by 40 percent by 2015 by addressing critical gaps in care during the most vulnerable time of life – the 1000-day window from conception, pregnancy, and birth of a baby, to the child’s second birthday. The emphasis of the program was on family planning, pre-and post-delivery care for mothers and newborns, immediate and exclusive breastfeeding, care and nutrition for children up to two years of age, and routine immunization. Coverage for treatment of diarrhea, pneumonia and some neglected diseases. An analysis to the program indicated that the use of the phones was eight times higher and that mothers were coming to the clinic due to the messages from the phones [23].
Mobile Technology for community Health (MOTECH) was an initiative of supporting providers and clients in Ghana in order to distribute health information to underserved populations by providing five keys functional mHealth areas including: behavior change and demand generation, management of patient data, workforce performance, last mile supply chain and patient adherence. An analysis of the program indicated that the messages often provoked behavior change, such as arriving early at the health center for delivery rather than waiting at the house. In maternal health care, it was noted that a relationship existed between women’s health and mobile technology [24]. They noted that, women with no mobile phone access, utilized fewer skilled obstetric services that led to less knowledge on maternal danger signs.
This proposal aims to provide standard information to the pregnant mother and her two gatekeepers (male and woman figure of the pregnant mother) in Kajiado Central County on safe motherhood throughout pregnancy through SMS on their mobile phones in order to support the pregnant mothers with the right information and encourage them to follow through with skilled birth utilization services. The proposed information will be in English, Swahili and/or native language throughout pregnancy time.
Policy guidelines checks
Kenya’s governors commitment to save lives of women and girls.
Fifteen governors from Mandera, Turkana, Wajir, Migori, Nakuru, Siaya, Kisumu, Nairobi, Homabay, Kakamega, Garissa, Marsabit, Taita Taveta, Isiolo and Lamu heed the clarion call “no woman should die while giving life” and boldly declared to promote safe motherhood in their respective counties. This was in relation to the UNFPA (2014) report that cited highest counties in maternal mortality. The Governors committed themselves to strengthening of partnerships with the Ministry of Health, the First Lady’s Beyond Zero Campaign, the United Nations Population Fund (UNFPA) and other stakeholders, to significantly reduce maternal deaths in Kenya. They acknowledged that the maternal mortality and morbidity problem was real in their respective counties and declared to work with urgency to reduce the rates. They described their commitment to empower women, embrace previous targets and strategies working towards reducing the rates, scale up the action irrespective of geographical location by improving the infrastructure. They committed to embrace the beyond zero campaign and support it in their counties, incorporate girl’s needs, increase investments in health, strengthen data collection, strengthen public private partnership and improve family planning and reduce poverty levels in their respective counties [11]. It is for this cause that this proposal wishes to ride on, in order to increase awareness to the gate keepers to hasten the achievement of safe motherhood one county at a time. Even though Kajiado was not part of the signatory, it has since been incorporated in the beyond zero campaign to enhance safe MNCH care. It is therefore timely and prudent to conduct this research in this county.
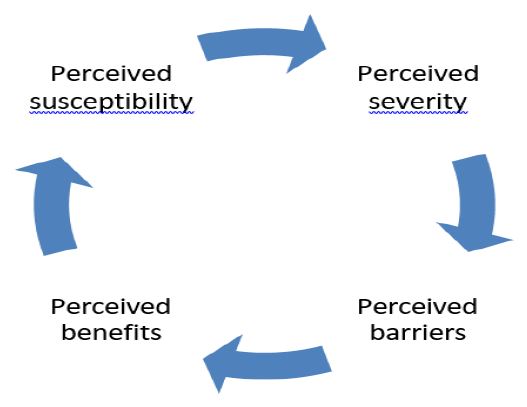
Health belief model
This model addresses the readiness to act upon health behavior that is linked to the individual’s health. It is a model that is suggested for health promotion programming. It involves four sections that can move in a cyclic way. This includes: perceived susceptibility, perceived severity, perceived barriers and perceived benefits.
Perceived susceptibility refers to beliefs concerning risk or susceptibility to a condition. In this study, perceived susceptibility will be highlighted as educating the mother who is pregnant and her household concerning safe motherhood throughout pregnancy. This information is important to both the mother and her household members that will be communicated through SMS on her mobile phone as well as her household member’s mobile phones. The information will be both educational as well as highlight the risk factors (increased morbidity and mortality of both the mother as well as the child). After perceived susceptibility is the perceived severity.
The perceived severity refers to beliefs concerning the maternal and neonatal health state. The believes include the cultural believes pertaining nutrition of a mother throughout MNCH continuum, her role in the family, the socioeconomic beliefs in the household that at times affect the utilization of MNCH throughout the continuum. Then, is the perceived barriers towards attaining safe motherhood in pregnancy during maternal and neonatal health continuum of care. These barriers might be antenatal related such as: financial implications for accessing maternal care on time, transport problems, delayed household decision making, lack of blood donor when in needed, delayed referral systems, poor nutrition, lack of accessing and utilizing the focused antenatal care services. Barriers might also be noted during labor and delivery or birthing time that might include: lack of a skilled birth attendant, lack of a birth companion, lack of information on danger signs, lack of information on pain management as well as lack of information on the birthing process and how to cope and adapt to it. Other services include targeted postpartum care services that are involved in taking care of both the mother and the child, encouraging acceptable infant feeding, rest for the mother, male involvement, vaccination, nutrition enhancement as well as progressive informational relationship with the health care providers till the next preconception time.
After perceived barriers, is the perceived benefits. The perceived benefits include having an empowered mother and her household members towards safe motherhood during pregnancy, strengthening the role of the man in pregnancy as well as the significant female in the family, acquiring a sense of satisfaction of the care, being preventers of complications, being contributors to safe motherhood during pregnancy and the ultimate goal of reducing morbidity and mortality in Kajiado Central in Kenya.
Source: Jones et. al., [25]
Research design
The study adopted a longitudinal study design approach. The women were followed from which ever gestational age at the point of contact till the end/termination of pregnancy. The pregnant women’s gatekeepers were given safe motherhood information at the same interval as the pregnant women so that they are aware of the information. Contacts from the pregnant mothers as well as their gatekeepers were obtained and sent the safe motherhood information through the SMS. The SMS were sent every two to three weeks after the first contact till the end of the pregnancy. However, the confirmation of receiving the messages or the reinforcement from the gate keepers were evaluated when the pregnant women come for their antenatal clinics as highlighted using the WHO FANC Model that illustrates the four visits as: 1st visit is between 8-12 weeks (during the first trimester), 2nd visit to be between 24-26 weeks, 3rd visit to be be at 32 weeks and 4th visit to be between 36-38 weeks (near the expected date of delivery).
Study site
The study was conducted in Kajiado County. Kajiado County is 80 kilometers south of Nairobi and it also borders Tanzania to the South. The county covers an area of 21,900 Km2. Kajiado county has 5 administrative sub counties namely, Kajiado central, South, North, West and East and also has 25 County Wards. Kajiado county was an estimated population of 999,819 in 2016/17 according to KNBS projections 2009. A rapid population and urbanization growth, estimates a Population of 1,200,000 in 2022 at annual growth rate of 5%. A high poverty rates and low literacy levels exposes a greater percentage of the population to various socio-economic risk factors. Kajiado county is largely Livestock and agriculture-based economy. The county has a referral hospital namely the Kajiado level four hospital. The study was conducted Kajiado central in Bissil Health centre. Umma University and Bisil Health centre have a collaboration of mentoring and instructing nursing students and therefore this was a viable site.
Study population
The study population was mothers who were pregnant, and living within the catchment area of Bisil Health center. These women were recruited from the health facility and their proposed gatekeepers. These gate keepers received safe motherhood information via their mobile phones on SMS platform as the participants did.
Sample size
Pregnant women of any stage of the pregnancy were be included in the study. Their significant female and male household persons were also included. The pregnant mothers were the contact person for the selected gatekeepers. The pregnant mothers were requested for their phone numbers after being well explained on the objectives of the study as well as her contacts. Each of the women signed written consents in order to participate in the study.
Calculation of a sample size
The formula (26) was used to approximate the sample size.
Where:
n=desired sample size when population >10,000
z=standard normal deviation at confidence level 95%=1.96
p=proportion in target population estimated to have characteristics of interest 55% (The Audience Scapes 2014) d=marginal error (5% or 0.05)
q= 1-p.
Therefore: 
=1.96² x0.55x0.45/0.05²
=3.8416x0.2475/0.0025
=0.950796/0.0025
=380 mothers
The final sample estimate formula:
nf= desired sample size for population less than 10,000
n= desired sample size when population> 10,000
N= estimate of population (pregnant women)
Substituting
nf= 380/1(380-1)/450
nf=380/1.86
nf=240 pregnant mothers
Sampling techniques
Purposive sampling was used for this research study. This sampling method was choosen because of the deliberate nature of the study.
Inclusion criteria of the principal participant
Pregnant mothers at any gestational age of the pregnancy
Pregnant mothers who will be able to communicate in Kiswahili or English.
Pregnant mother owning a mobile phone with an active line.
Pregnant mother who is above 18 years of age.
Pregnant mother who is recruited from Bisil Health Centre.
Suggested gatekeepers by the principal participant
The gatekeepers were suggested by the principal participant
The gate keepers were: one female and one male known to the participants.
The gate keepers (some) had a phone with an active line.
The gate keepers (some) could communicate to the pregnant mother in either English or Kiswahili or the mother’s native language.
The gate keepers (some) were willing and had given a verbal consent to be gate keepers to the pregnant mother.
Exclusion criteria for the principal participant
Pregnant mothers who did not consent for the study.
Pregnant mother without a personal phone with a nonactive line.
Data collection method
There will be various types of data which was in line with the study objectives, literature review and the frameworks.
Data collection tool
A questionnaire (appendix 1) was used to collect the data. It consisted of close ended questions written in English and translated to Kiswahili. Two research assistants were trained and recruited to assist in the recruitment process as well as the data collection process.
Data analysis
Data analysis was done using Statistical Package for Social Scientist (SPSS version 29). Relationships of the information received from the health care workers to the pregnant mothers and their gatekeepers was checked against the applicability of all the safe motherhood components throughout the MNCH continuum of care. Presentation of findings was done in form of tables, graphs and pie charts.
Pre-testing of instruments
Validity of the tools: Validity is the extent of accurate measurement of a concept. The researcher conducted a pre- test of the instruments. Validity of the questionnaire was done in-order to check whether the constructed questions were clear, suitable and easy to be understood by the pregnant mothers.
Reliability of the data collected: This is the accuracy of an instrument to give the same results if it is used in the same situation on repeated occasions. Cross checking of the instruments was done daily to ensure completeness before data entry. Research assistant was trained prior to the data collection process and they were also involved in the pre- test of the questionnaire. The researcher was not able to supervise the assistants during the data collection period due to the country’s lockdown but online briefing was done every week.
Ethical consideration
Prior to the study, ethical approval was sought from Nacosti, Kajiado County Health Department in conjunction to Bisil Health Center. Approval for the research was also sought from research department - Umma University Ethical Review Committee.
All respondents were informed that their participation was voluntary and that the data collected would only be used for the purpose of the study, for their benefit. Their privacy and confidentiality were affirmed by entering into a consent agreement in Appendix 1 and 2.
The data collection was undertaken during the covid 19 pandemic (2020-2021) when the country was under lockdown and access to the health facility was limited. However, clients were encouraged to access essential services as the health care providers still remained available to offer care. However, it was observed that the attendance to the facility greatly declined. The projected sample size at the time of proposal was 240 pregnant mothers. However, only 49 (20%) mothers accessed the facility and were followed up until they delivered.
Demographic data
The demographic of the women interviewed revealed that 40.8% (n=20) were gravida 1, 26.3% (n=13 ) were gravida 2, 8.1% (n=4) were gravida 3, 14.2% (n=7) were gravida 4, 6.1% (n=3) were gravida 5 while 2.0% were gravida 7 and 8. While asked about their parity, 24.4% (n=12) were nulipara, 38.7% (n=19) were para 1, 10.2% (n=5) were para 2, 22.4% (n=11) were para 3, 4.0% (n=2) were para 4. When their educational background was sought, 10.2% (n=5) had primary education, 46.9% (n=23) had secondary education, 32.6% (n=16) had tertiary educanntion, 8.1% (n=4) had informal education while 2% (n=1) had no education. For the source income, 53% (n=26) were business women, 12.2% (n=6) were teachers, 26.5% (n=13) were farmers, 4% (n=2) were police officers while the rest reported to receive money from their parents for upkeep. This information is represented by (Table 1) below.
| Gravity | Frequency | % | Parity | Frequency | % |
|---|---|---|---|---|---|
| 1 | 20 | 40.8% | 0 | 12 | 24.4% |
| 2 | 13 | 26.5% | 1 | 19 | 38.7% |
| 3 | 4 | 8.1% | 2 | 5 | 10.2% |
| 4 | 7 | 14.2% | 3 | 11 | 22.4% |
| 5 | 3 | 6.1% | 4 | 2 | 4.0% |
| 7 | 1 | 2.0% | 5 | 0 | 0% |
| 8 | 1 | 2.0% | 6 | 0 | 0% |
| Total | 49 | 100 | Total | 49 | 100 |
| Educationbackground | Frequency | % | Source ofincome | Frequency | % |
| Primary | 5 | 10.2% | Business | 26 | 53.0% |
| Secondary | 23 | 46.9% | Teacher | 6 | 12.2% |
| Tertiary | 16 | 32.6% | Farming | 13 | 26.5% |
| Informal | 4 | 8.1% | Police | 2 | 4.0% |
| No knowneducation | 1 | 2.0% | Money fromparents | 2 | 4.0% |
| Total | 49 | 100% | Total | 49 | 100% |
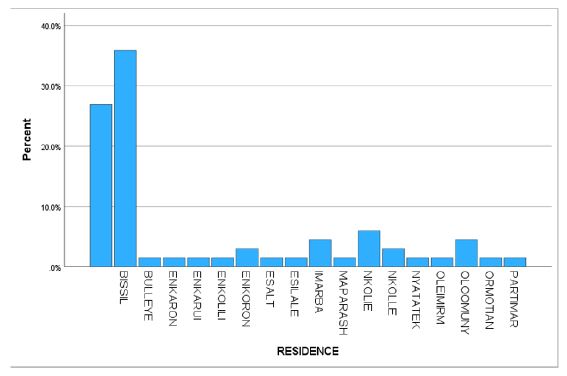
Proximity/residence to the facility
When asked about their residence, close to half 44.8% (n=22) women resided in Bissil location which was a 10 minutes’ walk, 12.2% (n=6) from Nkolie, Enkoron, Imarba, Oloomuny were approximately 30 minutes’ walk to Bissil facility, while 4% (n=2) was a 1 hour walk which was 1% each from Bulluye, Enkarui, Enkolili, Esalt, Esilale, Maparasha, Nyatatek, Ormotian, and Partimar. This is represented in Figure 1.
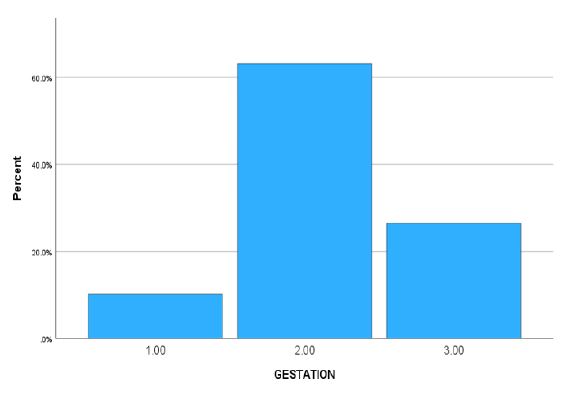
Gestation of the women who accessed antenatal care
Among the women who were in the study, many 63.2% (n=31) were in the 2nd trimester, afew 26.5% (n=13) in the third trimester while some 10.2% (n=5) in the first trimester. As illustrated in Figure 2.
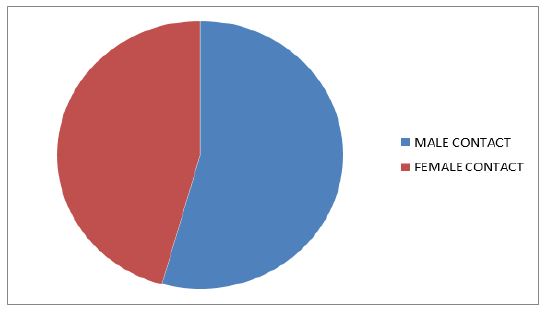
Phone contacts
Among the 49 women who were interviewed, majority 91% (n=45) were married while 8% (n=4) were not married. Among the women, 97% (n=48) gave a male contact number while only one woman did not give a male contact number. When asked to give female contact number, 81.6% (n=40) of the women gave a female contact number. This is represented in Figure 3.
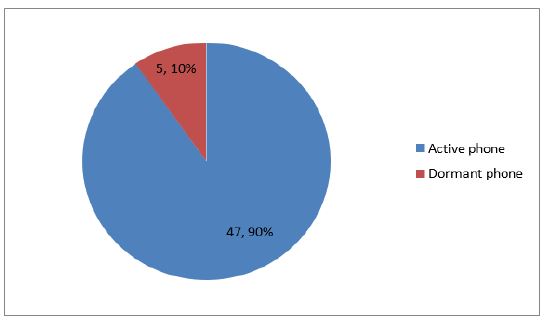
Active phones vs dormant phones
The women were asked if they were in possetion of a phone and if it was working. Majority 90% (n=47) of the women had active phones while 10% (n=2) of the womens phone was not working. This information is illustrated in Figure 4.
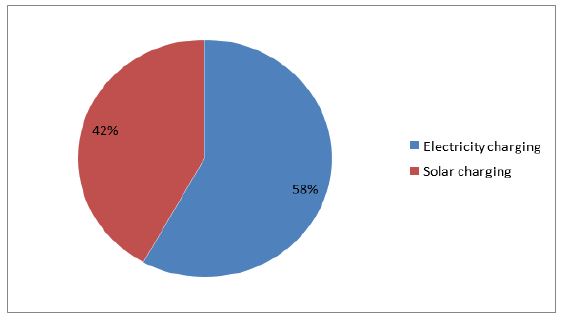
Phone charging
Since majority of the women owned phones and they were active, they were asked how they charged their phones. Twenty nine 59% charged their phones with electricity while 41% (n=20) charged their phones using solar as shown in Figure 5.
Network availability
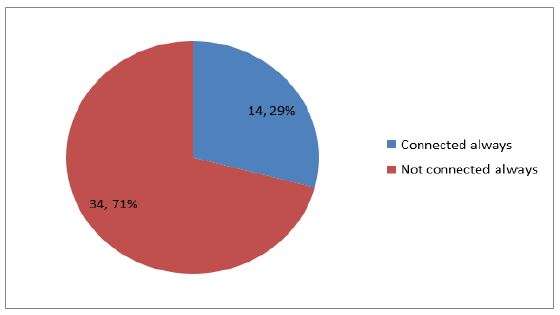
When asked if they had frequent network connectivity, Majority 69% (n=34) stated that they did not have frequent network connectivity while 28.6% (n=14) stated that they frequently had network connectivity as illustrated in Figure 6.
Service preference
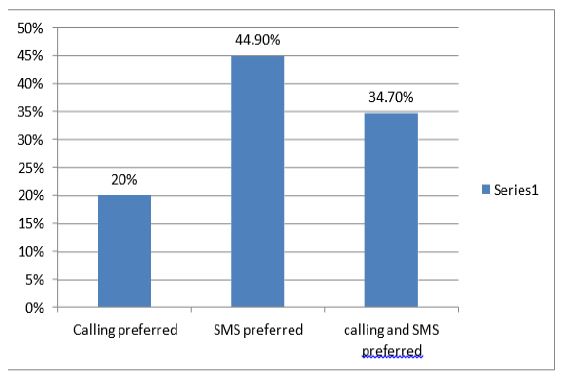
After enrollment, the mothers were to receive antenatal messages. Therefore, as they were being enrolled, they were asked the most preferred service between (Short Message Service) SMS or calls. Notably, 44.9% (n=22) preferred SMS communication of health messages, 34.7% (n=17) preferred both SMS and calls while 20.4% (n=10) preferred being called as represented by Figure 7.
Number of messages the women received
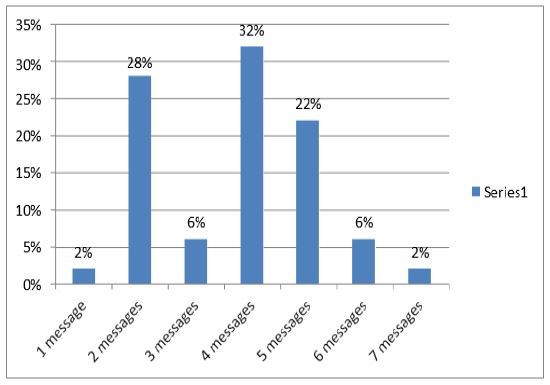
As the women accessed the antenatal care, health care messages were given. 32% (n=16) received 4 messages, 28% (n=14) received 2 messages, 22% (n=11) received 5 messages, 6% (n=3) received 3 messages as well as 6 messages while 2% (n=1) received 1 and 7 messages as represented in Figure 8 below.
Womens delivery of their babies in facilities
As the women received at least an SMS, it was also noted that all of the women delivered in the facility with skilled birth attendants except for one mother who delivered on her way to the facility.
Discussion of received messages among male stakeholders and their women.
The essence of sharing messages with both male and female caretakers was to encourage discussion of the received messages so as to ensure an impacted outcome. Among all the men who received similar messages as the women, 85.7% (n=42) reported to have discussed the received message with their women while 14.2% (n=7) did not discuss the messages.
The clients who were included in the study were 49 (20%) amidst a prospective 240 mothers. This revealed an approximate 80% decrease of the outpatient utilization of service due to Covid pandemic lockdown. A 20% decrease to outpatient facility was also noted in some Kenyan hospitals [27] while others recorded a universal outpatient decline ranging from 10% to 91% [28]. This revealed a worrying trend in the event of disruption of traditional health care trends This therefore calls for innovative modes from the face-to-face traditional consultations and interactions.
Concerning the distance and accessibility to the facility, it was evident that close to half of the women who accessed the facility had to walk for at least 10 minutes. However, some women had to walk for 30 minutes and others more than one hour. Apparently, the locations that were 1 hour radius from the facility had fewer women. This finding revealed the challenges of accessibility since an estimated hour of walking suggested more than 5 kilometers distance which discouraged access to the facility [29]. The country wide lockdown seemed to have exposed this truth among the pregnant women. Therefore, maternal services should be made accessible with this information in mind.
Most of the women who were accessing antenatal care were in the 2nd trimester while a few were in the first trimester. This information revealed that most women did not acknowledge the importance of accessing antenatal care in the first trimester but rather started in the second trimester [30]. Some of the reasons for the delays were: lack of knowledge on advantages of first trimester access, first trimester discomforts, or sometimes the advice pregnant women got from their friends and relatives. It is therefore important to advice women and their stakeholders of early first trimester access so as to curb some complications early and enhance woman skilled birth relationship.
Since the study was about utilization of health information on mobile phone services for implementation of safe motherhood, the women were asked to give one preferred male and female contact number. Notably, more male numbers were given than the female numbers. This affirmed the confidence the pregnant women had on the role of the man in an African family. Apparently, this confidence bestowed on the man seemed to play a significant role in maternal care especially during decision making and avoiding delays that would lead to maternal mortality [31]. This male involvement should therefore be encouraged and highlighted in all maternal health engagements. Among the women in the study, majority of them had an active line and phone. This resonated with GSMA statistics of an achieved 80% penetration in Kenyan population [32]. This was very encouraging as it even revealed an anticipated projection of 7 million by 2025. This will therefore place Kenya among highly mobile technology penetration in the Sub-Saharan Africa. This therefore gives room for innovative mobile health exploration, utilization and sustainability in the Kenyan health care population.
As the women owned mobile phones, they charged their gadgets using electricity or solar charging systems or at times both. Notably, majority of clients had access to electricity charging system, with solar charging gaining popularity. The solar system can therefore be encouraged especially on remote areas as it could save on electricity expenses, it was cheap, and had lower production costs [33].
Even with availability of phones, majority of women and men sometimes experienced low network connectivity. However, even with low connectivity, households would still access the health information. This was made possible since during lockdown, the men would travel to centers to get food or essential supplies for the family and therefore enhance their connectivity altogether. They therefore returned home with essential supplies as well as health messages on their phones. Low network connectivity should therefore be noted and improved especially with the advent of mHealth integration [34]. An intersectoral collaboration between technology and health should be highlighted so that women and family benefit from their engagement and health promotion.
The most preferred mobile service was the Short Message Service (SMS). This was impactful [35] because it is a good point of reference and would be discussed or referred to without being altered. Likewise, the short messages did not require internet or web connectivity or loggings especially to simple phones [36]. The dispatch of health messages should therefore be encouraged on all settings even if advanced internet connectivity is scarce.
Throughout the research process, majority of women and the men received an average of 3 messages. Consequently, positive outcome where women delivered in the facility with skilled birth attendants was experienced. This was encouraging because communication channels were kept open and encouraged between the household and the skilled birth attendants despite the COVID lockdown. This revealed that positive response to health care and positive behavior might be enhanced with innovative, and repetitive engagements [41] between all stakeholders.
It was evident that mHealth is a service that needs to be embraced in this day and age. The Covid 19 pandemic revealed hiccups to noncompliance to mHealth in our country and globally especially in the rural environments. However, it was encouraging to note that all the women who were followed up through mobile tracking and health messaging, appreciated as well as their gatekeepers and had good outcomes. It is therefore of great importance that telecommunication is embraced in health care by enhancing connectivity for better health facilitation.
