ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1UCMS & GTBH, Dilshad Garden, India.
2NCDC, Sham Nath Marg, India.
UCMS & GTBH, Dilshad Garden, India.
Email: shyamadutt0@gmail.com
Received : Feb 14, 2025,
Accepted : Mar 12, 2025
Published : Mar 19, 2025,
Archived : www.jclinmedcasereports.com
The prevalence rate of superficial fungal infection differs from place to place according to environmental condition and also due to poor hygienic condition of population. Dermatophytes are mycelial group of closely related keratinophilic fungi, originally saprobial. This is a fundamental mechanism observed in Trichophyton rubrum and Trichophyton mentagrophytes in establishing superficial infection. Proteases and keratinases are expressed by common dermatophytes: Trichophyton rubrum and Trichophyton mentagrophytes which have optimum activity at acidic pH values, and are able to establish contact with human acidic skin due to the environment. These are identified by molecular and conventional method. Out of 60 culture positive patients included skin and nail also, 43.34% cases were naïve, reported infection for the first time; 50% cases were on antifungal treatment for 1-2 years and 6.66% cases were with recurrence’s which were presenting with lesions at the same or different site after completion of previous therapy. These were categorized as naïve, recalcitrant and reinfection respectively. According to the profile of various dermatophytosis patients studied till now mean age of dermatophytosis patients was 30.02±10.95, with a male/female ratio of 40/20. All the patients with dermatophytosis were tested for dermatophytic infection, out of 200 samples that were hyphae +ve by KOH only 140 isolates were culture positive. Among them only 60 isolates were positive for Trichophyton. Further, only 20 strains are positive for T. rubrum & 40 strains are positive for T. mentagrophytes, which were also confirmed by PCR & sequencing using species specific ITS 2 primer of T. rubrum & T. mentagrophytes complex.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Datt S (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Dermatophytes are keratinophilic fungi that cause superficial fungal infection; grow on skin, mucous membranes, hair and nails. Dermatophytes are not a part of the normal human microbial flora but are well adapted to host keratin utilizing it as a source of nutrition for establishing infection [1].
The prevalence rate of superficial fungal infection differs from place to place according to environmental condition and also due to poor hygienic condition of population. In India most of the places are very hot and humid climate because of that our country has more prevalence rate of superficial fungal infections [2-4]. In spite of therapeutic advances in the last decades, the prevalence of cutaneous mycoses is still increasing [5]. Most of the people are living in very low socioeconomic status, crowded living environment, and poor medical care and wearing of dirty clothing which adds to the increased prevalence of cutaneous fungal infections [3]. This infection does not cause any death but it may lead to morbidity and plays a more important role in health-related problems. Dermatophytes are mycelial group of closely related keratinophilic fungi, originally saprobial. Dermatophytoses is also termed as Tinea and the clinical conditions are named as “Tinea” followed by the anatomical site of infection in latineg., tinea capitis, tinea corporis, and tinea pedis etc.
Dermatophytes comprise of 52 species of keratin degrading ascomycetes belonging to genera Trichophyton, Microsporum, Epidermophyton, Arthroderma, Lapophyton, Nanninzia, Ctenomyces, Guarromyces, Paraphyton. But human dermatophytosis is caused primarily by Trichophyton rubrum (T. rubrum), Trichophyton mentagrophytes (T. mentagrophytes), Trichophyton interdigitale, Epidermophyton floccosum and Microsporum canis and others. Globally Trichophyton rubrum commonly causes 50–80% of onychomycosis and tinea pedis but in India Trichophyton mentagrophyte is more prevalent in Tinea corporis and Tinea cruris [2].
During the initial stages of the infection, dermatophytes facilitate adhesions on host cell. It is initiated by a specific interaction of carbohydrate-binding proteins (lectin) with sugar (Sialic acid) as a terminal carbohydrate on the surface of the human cell. Proteases and keratinases are expressed by common dermatophytes: Trichophyton rubrum and Trichophyton mentagrophytes which have optimum activity at acidic pH values, and are able to establish contact with human acidic skin due to the environment. The secretion of these proteases and peptidase, have been identified as an important step in fungal pathogenicity and virulence. The metabolism of some amino acids shifts the extracellular pH from acidic to alkaline values at which most known keratinolytic proteases have optimal enzymatic activity. This is a fundamental mechanism observed in Trichophyton rubrum and Trichophyton mentagrophytes in establishing superficial infection [3].
Their ability to utilize keratin as major nutrient source and high affinity for keratin facilitates them to invade keratinized structures like nails, skin and hair causing superficial infections known as dermatophytose s in humans and animals. This is commonly known as ring worm infection. The infection is generally cutaneous and restricted to the nonliving cornified layers as the fungi is unable to penetrate the deeper tissues or organs of immunocompetent hosts.
The clinical isolates were collected for a period of four years, from August 2015 to July 2019. All the samples (n=280) received in the mycology laboratory from Out Patient’s Department (OPD) of tertiary care Guru Teg Bahadur hospital, Delhi. Institutional ethical committee approval was obtained prior to commencement of the study. Written informed consent was taken from each participant. The patient information sheet for participation in the research project was provided to each participant.
Clinical sample collection
Scrappings were collected from the affected nail and skin surface of patients referred from OPD with suspected dermadermatophytosis. The affected sites were decontaminated with 70% alcohol and the nail clippings from the discolored, thickened nail bed, or nail plate was collected. The skin sample was taken from the advancing edge of lesions by scraping from the center to edge using a sterile scalpel Samples were divided into two portions for direct microscopy and fungal culture.
Microscopic identification
Microscopic identification of the samples were done using 40% Potassium Hydroxide (KOH) The specimen was briefly heated and then observed microscopically under 40X magnification. The presence of fungal hyphae, arthroconidia, was considered as a positive result for suspected dermatophyte infection.
Phenotypic confirmation of the species
A portion of the samples were cultured on Sabouraud’s Dextrose agar (Hi-media, Mumbai) with antibiotics such as chloramphenicol (0.05 gm/l), Gentamicin (20 mg/l) and Cyclohexamide (0.5 gm/l) (Hi-media, Mumbai). All inoculated tubes were incubated at 25°C for 3-4 weeks till optimal growth. After the growth, the etiological agent was confirmed by characteristic morphology of colony (pigmentation of the surface and reverse side, topography, texture and the rate of growth) and by studying the microscopic appearance of fungus on LPCB mounts. The species were confirmed by size and shape of macro conidia, microconidia, spirals, nodular organs and pectinate branches [1].
Genotypic confirmation of the species
These isolates were further confirmed by PCR and sequencing using species specific primers of Trichophyton rubrum and Trichophyton mentagrophytes [2].
DNA extraction
DNA was extracted from the cultures grown on SDA by using commercially available DNA extraction kit (Hi Yield genomic DNA kit, RBC, Taiwan).
Polymerase chain reaction (PCR)
On the basis of sequences of internal transcribed spacer to in NCBI nucleotide data base primer of Trichophyton rubrum and Trichophyton mentagrophytes were used shown in table-1 and the PCR product length of two primer sets were 203 base pair and 130 base pair respectively. For PCR each tube contained a total volume of 25 μl mix including 2.5 μl buffer (10X), 5 μl of Q-buffer, 0.5 μl dNTPs (200 μM), MgCl2 0.5 μl (1.5 mM), 0.15 μl Taq polymerase, 1 μl of each primer, forward and reverse (10 μM), 5 μl of the extracted DNA and nuclease free water to make up the volume. All PCR reagents were purchased from Qiagen, and amplification was performed on a thermo-cycler (Eppendorf) at the thermal profile shown in table 2 and 3 [3,4]. Standard ATCC control strains were used as positive controls (T. mentagrophytes ATCC. 28185) [5].
| S. No. | Region | Primername | Primer sequence |
|---|---|---|---|
| 1 | ITS 2 | *TR F | F 5′ TCTTTGAACGCACATTGCGCC 3′ |
| TR R | R 5′ CGGTCCTGAGGGCGCTGAA 3′ | ||
| 2 | ITS 2 | *TM F | F 5′-CAAACGTCCGTCAGGGTGAGC 3′ |
| TM R | R 5′-TAGCCACTAAAGAGAGGCTCGC 3′ |
| Temperature | Time | Cycles | Phase |
|---|---|---|---|
| 95°C | 10 min | 1 | Initial Denaturation |
| 95°C | 60 sec | 35 | Denaturation |
| 60°C | 45 sec | Annealing | |
| 72°C | 60 sec | Extension | |
| 72°C | 7 min | 1 | Final extension |
| 4°C | ∞ | 1 | Hold |
| Temperature | Time | Cycles | Phase |
|---|---|---|---|
| 95°C | 10 min | 1 | Initial Denaturation |
| 95°C | 60 sec | 35 | Denaturation |
| 65°C | 30 sec | Annealing | |
| 72°C | 60 sec | Extension | |
| 72°C | 7 min | 1 | Final extension |
| 4°C | ∞ | 1 | Hold |
The amplified PCR products were analyzed by electrophoresis on 1.2% agarose gel, at 125 V and 15 mA current in 10 slot apparatus for 40 minutes, stained with Ethidium Bromide.
Sequencing
Purification of the PCR product was done using Gel purification kit protocol (Qiagen, Germany). Sequencing was done as per protocol used by big dye terminator method followed by Sanger sequencing method. The sequence analysis was performed by comparison of the nucleotide with dermatophyte reference nucleotide sequences obtained from the gene bank data base (http://www.ncbi.nih.gov/gene), match sequence with data base and submit the sequence in gene bank data base for the accession number.
Statistical analysis
Bionumerics software (Applied Maths and Ghent) was used for consensus and concatenation of the sequences. The sequences and amino acid sequences depicted by using the ExPASy online tool (https://web.expasy.org/ translate/) were aligned.
Identification of culture
→ A total of 280 samples were collected, which included 120 onychomycosis and 160 tinea infection.
→ Out of 120 nail samples, 90 were found to be KOH positive, and 60 samples were culture positive for dermatophytes and non-dermatophytes.
→ Among 60 isolates from nail sample (Figure 1), 19 isolates were identified as T. rubrum and 5 isolates as T. mentagrophytes complex.
→ Similarly, of 160 skin samples, 110 cases were observed as KOH positive, of which 80 samples were culture positive. Of 80 culture isolates 35 isolates were characterized as T. mentagrophytes complex and 1 isolate as T. rubrum.
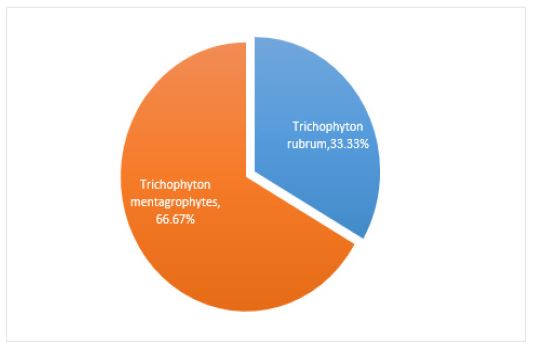
→ A total of 60 culture isolates (nail and skin) as confirmed by LPCB, PCR and reconfirmed by sequencing, 40 isolates are of T. mentagrophytes complex and 20 isolates are of T. rubrum shown in figure 2.
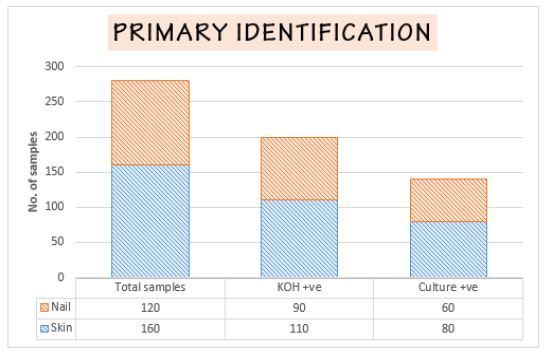
| Cases | Total Cases | Skin (%) | Nail (%) |
|---|---|---|---|
| Total Cases | 280 | 160(57.14%) | 120(42.86%) |
| KOH positive | 200 | 110(55%) | 90(45%) |
| Culture positive | 140 | 80(57.14%) | 60(42.86%) |
| T. mentagrophytes | 40 | 35(87.5%) | 5(12.5%) |
| T. rubrum | 20 | 1(5%) | 19(95%) |
Phenotypic distribution of isolates
In this study, a total of 280 samples suspected of dermatophytosis were collected, with 200 samples confirmed by KOH for fungal elements (110 cases of Tinea and 90 of onychomycosis).
From 110 Tinea cases 80 were found to be culture positive similarly out 90 onychomycosis cases 60 cases were culture positive.
→ The patients mean age with standard deviation was 32.51±11.32 years. The duration of dermatophytic infection in the cases ranged from 3 months to 10 years (9.8 months±5.45 months).
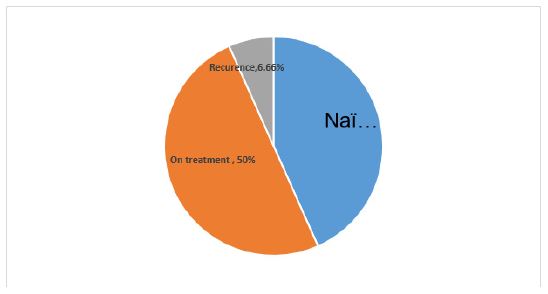
→ Out of 60 culture positive patients included skin and nail also, 43.34% cases were naïve, reported infection for the first time; 50% cases were on antifungal treatment for 1-2 years and 6.66% cases were with recurrence’s which were presenting with lesions at the same or different site after completion of previous therapy. These were categorized as naïve, recalcitrant and reinfection respectively (Figure 3).
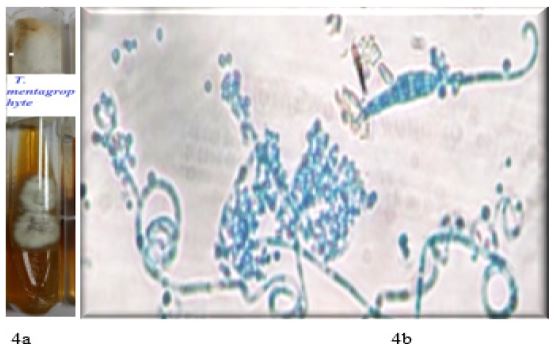
Phenotypic characteristics of Trichophyton mentagrophytes
Microconidia of Trichophyton mentagrophytes complex were spherical, sessile, arranged in dense, grape-like clusters or along the hyphae. Macroconidia were 3-8 celled, smooth and thin walled, clavate to cigar-shaped (Figure 4a & 4b).
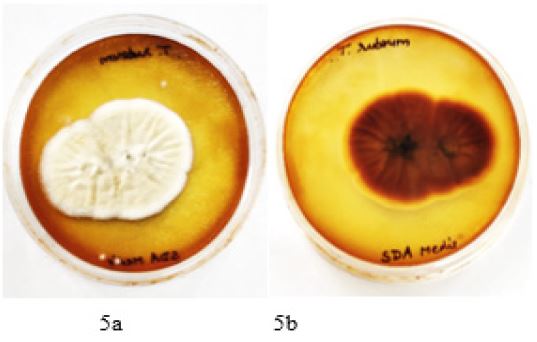
Phenotypic characteristics of Trichophyton rubrum
Colonies were fluffy to cottony, white and most of the isolates turned rose when aging, reverse showed wine red pigmentation (Figure 5). Macroconidia seen occasionally, but when present are thin walled, poorly differentiated with variable size cylindrical to cigar-shaped. Microconidia were peg-shaped to pyriform. Sessile alongside undifferentiated hyphae (Figure 5a & 5b).

All isolates were subjected to PCR using species specific primer of the ITS region for further confirmation.
Clinical manifestation
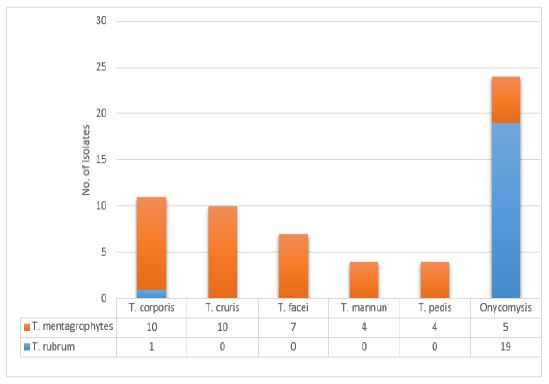
Amongst the 60 isolates, tinea corporis was predominant clinical presentation in 11 cases (18.33%) followed by T. cruris 10(16.67%), T. facei 7(11.67%) and T. pedis in 4(6.67%) (Figure 7). T. mentagrophytes complex was the major causative agent except in one case of T. corporis, T. rubrum was isolated on culture. While in 24 (40%) cases of onychomycosis, T. rubrum 19/24(79.17%) was isolated followed by T. mentagrophytes complex in 5 cases (20.83%).
| Age Group(years) | Trichophyton mentagrophytes complex | Trichophyton rubrum | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | |||||
| Skin | Nail | Skin | Nail | Skin | Nail | Skin | Nail | |
| 20- Oct | 8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 21- 30 | 8 | 1 | 2 | 0 | 0 | 7 | 0 | 4 |
| 31- 40 | 6 | 1 | 5 | 1 | 0 | 2 | 1 | 0 |
| 41- 50 | 2 | 0 | 2 | 2 | 0 | 1 | 0 | 2 |
| 51- 60 | 1 | 0 | 1 | 0 | 0 | 3 | 0 | 0 |
| Total | 25 | 2 | 10 | 3 | 0 | 13 | 1 | 6 |
The site of infection are shown in Figure 6a- 6d before isolation of T. rubrum and T. mentagrophytes complex.
Age distribution
The prevalence of Dermatophytic infection was more common in male patients 40/60 (66.67%) as compared to female patients 20/60 (33.33%) in both onychomycosis and Tinea infection.
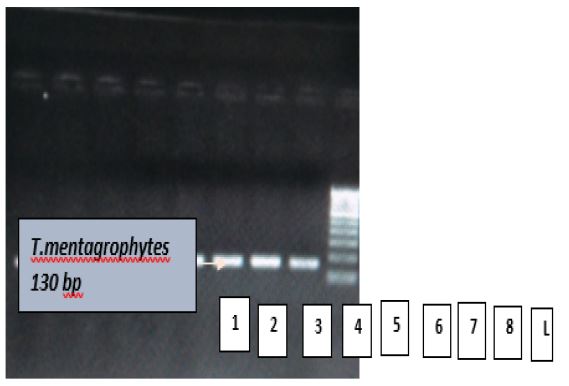
Genotypic confirmation of Trichophyton mentagrophytes by PCR: Figure 8a showing Lane 1-8 and L (ladder). Where lane 1-8 showing bands of samples of T. mentagrophytes, and L is 100 base pair molecular weight marker (Fermentas).
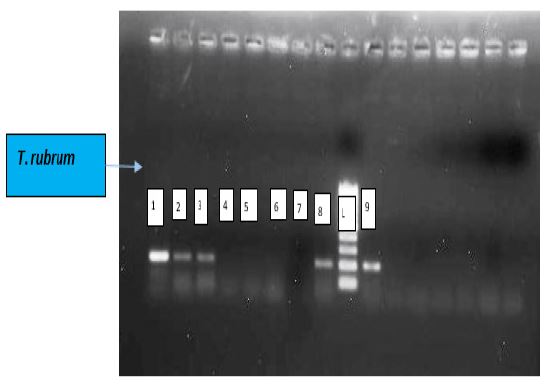
Genotypic confirmation of trichophyton rubrum by PCR: Figure 8b showing Lane 1-7, L (ladder) and 8. Where Lane 1-3, 7 & 8 are samples of T. rubrum, Lane 4-6 are negative control (no template) and L is 100 base pair molecular weight marker (Fermentas).
Sequencing
Purification of PCR products was done by Sodium Acetate Manual method and DNA sequence analysis was performed and by comparison of the nucleotides with dermatophytes reference nucleotide sequences obtained from the gene bank database (http://www.ncbi.nih.gov/gene), T. mentagrophytes and Trichophyton rubrum were showing 99% similarity with the reference strain. The representative sequence obtained were submitted to the gene bank database; and Accession numbers were obtained, total sequence submitted 12 numbers that are T. mentagrophytes accession no. are (9 sequences) MW497552 to MW497560, (3 sequences) MH644185, MH745112 & MH778308. and total sequence submitted 19 numbers that are Trichophyton rubrum accession no.- (16 sequences) MW506332 to MW506347 and (3 sequences) MH497367 to MH497369.
Figure showing Electropherogram of T. mentagrophtes
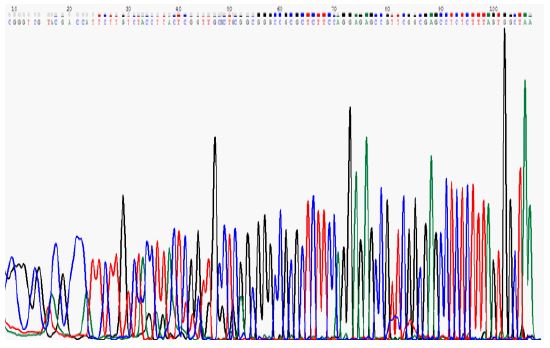
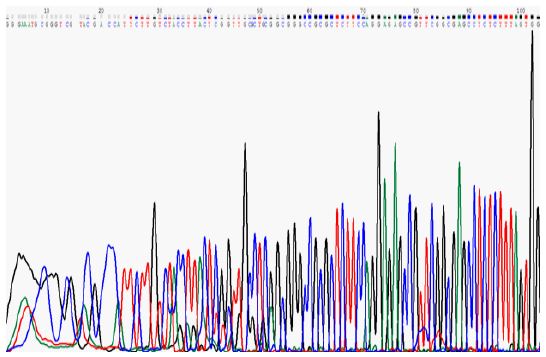
Figure showing Electropherogram of T. rubrum
According to the profile of various dermatophytosis patients studied till now mean age of dermatophytosis patients was 30.02±10.95, with a male/female ratio of 40/20. All the patients with dermatophytosis were tested for dermatophytic infection, out of 200 samples that were hyphae +ve by KOH only 140 isolates were culture positive. Among them only 60 isolates were positive for Trichophyton. Further, only 20 strains are positive for T. rubrum & 40 strains are positive for T. mentagrophytes, which were also confirmed by PCR & sequencing using species specific ITS 2 primer of T. rubrum & T. mentagrophytes complex.
The present study was conducted in patients with dermatophytosis with a mean duration of the disease as 8 months to 5 years attending the dermatology OPD of our tertiary care hospital in East Delhi. Chronic dermatophytosis has emerged as a vast problem in India with several cases of reinfection and relapse with failure to treatment being reported across the country. The geographical condition of this part of our country being hot and humid, makes it favorable for the development of superficial fungal infections [15]. Besides conductive environment other factors that aid these infections include unhygienic living condition, high population density, and application of steroids, incomplete treatment and probable drug resistance.
As documented in other studies, males appeared to be more exposed and acquire dermatophytic infection (58.3%) as compared to females (41.7%) which is in accordance to the other researchers worldwide [16,17]. Previously published data shows that the highest prevalence of dermatophytic infection in the 21-30 age group well understood as males are involved in outdoor activities in Delhi [18,19].
We found in our study that T. mentagrophytes was more prevalent than T. rubrum Delhi, which is also supported by the studies done by Patel P et.al 2010 [14].
