ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Philadelphia College of Osteopathic Medicine, Philadelphia, PA, USA.
2Department of Ophthalmology, Trinity Health Mid-Atlantic, Nazareth Hospital, Philadelphia, PA, USA.
3IC Laser Eye Care, Bensalem, PA, USA.
Department of Ophthalmology, Trinity Health Mid-Atlantic, Nazareth Hospital, Philadelphia, PA, USA.
Tel: +1 (215) 639-4500;
Email: Behnam.Rabiee@gmail.comEmail: arturogiordano@tin.it
Received : May 18, 2025,
Accepted : Jun 20, 2025
Published : Jun 27, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rabiee B (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
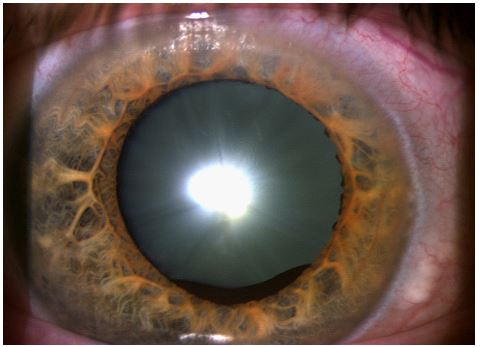
Iris cysts are uncommon but clinically important lesions that can present in both pediatric and adult populations. They may be either primary or secondary in origin and can lead to a range of ophthalmic complications. Although frequently benign and asymptomatic, certain cysts, particularly those impinging on the visual axis, can result in significant visual impairment. Pediatric patients are especially vulnerable, with a higher risk of developing amblyopia or strabismus due to prolonged visual axis obstruction [1-3]. Other notable complications include corneal decompensation from prolonged contact, inflammatory sequelae such as secondary uveitis, and increased intraocular pressure resulting in secondary glaucoma [1-4].
The goal of management is to minimize visual impairment while reducing the risk of recurrence and iatrogenic complications. Clinical strategies must therefore be tailored based on the lesion’s size, location, type, and symptomatology. This brief review provides original images and outlines the complications associated with iris cysts, evaluates contemporary management strategies, and highlights key considerations in distinguishing iris cysts from iris melanoma.
The potential complications associated with iris cysts are multifaceted. Obstruction of the visual axis can cause amblyopia or strabismus in younger patients due to disrupted visual development [1,3]. Corneal decompensation may ensue when prolonged contact between the cyst or the overlying iris and corneal endothelium leads to edema and endothelial cell loss [1,2]. Additionally, the presence of a cyst can initiate intraocular inflammation, manifesting as secondary uveitis [2]. Angle closure due to cyst-induced anatomical changes may elevate intraocular pressure, predisposing patients to secondary glaucoma [2,4].
| Feature | Iris cyst | Iris melanoma |
|---|---|---|
| Border | Smooth, well-circumscribed | Irregular, poorly defined |
| Translucency | Translucent or semi-translucent | Opaque, solidappearance |
| Vascularity | Avascular | Intrinsic vascularity; may showtortuous or leaky vessels |
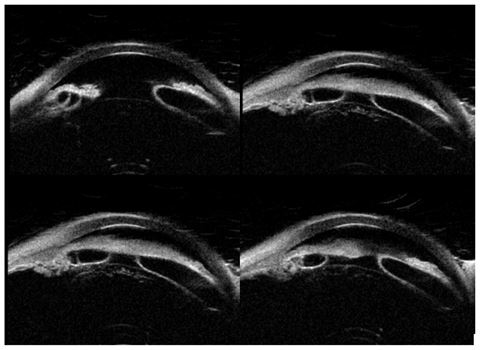
| ImagingFeatures | Thin-walled, fluid-filled lesion;low internal reflectivity on UBM or AS-OCT | Solid mass; medium to high internal reflectivity; shadowingon UBM |
| Treatment Approach | Observation, aspiration, lasertherapy, or excision if symptomatic | Surgical excision, plaquebrachytherapy, or enucleation depending on stage |
| Step | Management strategy | Indications |
|---|---|---|
| 1. Observation | - Periodic monitoring with slit-lamp and imaging (e.g.,UBM, AS-OCT) | - Asymptomatic- Stable primary pigment epithelial cysts- No visual axisobstruction |
| 2. Aspiration | - Fine-needle aspiration under slit-lamp or intraoperatively | - Symptomatic cysts- Progressive enlargement- Visual axis involvement |
| 3. Sclerotherapy | - Injection of absolute alcohol or mitomycin-C intocyst cavity post-aspiration | - To reduce recurrence after aspiration, particularly in stromal or recurrent cysts |
| 4. Laser Therapy | - Argon laser photocoagulation- Nd:YAG lasercystotomy | - Cysts refractory to aspiration- Thin-walled cysts amenable to collapse |
| 5. Surgical Excision | - Iridectomy or iridocyclectomy-May use vitrector or microdiathermy adjuncts | - Persistent, recurrent, or complex cysts-Failure of less invasive treatments- Diagnostic uncertainty |
| 6. SpecialConsiderations | - Avoid over-treatment in asymptomatic patients- Confirm diagnosis to rule out iris melanoma with imaging | - Inconclusive imaging- Rapidgrowth, irregularity, or vascularization requiring biopsy or excision |
Management of iris cysts is largely dependent on symptom burden and cyst morphology. Asymptomatic primary pigment epithelial cysts typically require no intervention and are managed conservatively with periodic observation [2,3]. For symptomatic lesions, fine-needle aspiration represents a common initial approach. Adjunctive use of sclerosing agents such as absolute alcohol or mitomycin-C has demonstrated efficacy in preventing recurrence [1,2,5].
Laser therapies, including argon and Nd: YAG modalities, offer non-invasive alternatives for cyst collapse in refractory cases or when aspiration is insufficient [2,4]. When non-surgical measures fail, surgical excision through iridectomy or iridocyclectomy may be indicated, particularly for persistent or visually compromising cysts [1,3,6]. Newer adjunctive interventions, such as microdiathermy at the cyst base and use of vitrectomy cutters for wall removal, aim to minimize recurrence and preserve adjacent ocular structures [1,7].
Accurate differentiation between iris cysts and iris melanoma is essential due to their vastly different clinical implications and management pathways. Iris cysts are typically benign, fluid-filled, and may be congenital or acquired due to trauma or inflammation. They usually appear translucent on slit-lamp examination and are best characterized using imaging modalities such as Ultrasound Biomicroscopy (UBM) and Anterior Segment Optical Coherence Tomography (AS-OCT) [1-3]. In contrast, iris melanoma arises from melanocytes and typically presents as a solid, pigmented lesion with irregular borders, intrinsic vascularity, and potential for local invasion and metastasis (Table 1). Diagnostic imaging and fluorescein angiography assist in assessing vascular characteristics and internal reflectivity. Unlike cysts, melanomas often display tortuous, leaky vessels and require more aggressive management, including excisional biopsy, plaque brachytherapy, or enucleation in advanced stages [4-7].
In summary, Iris cysts, while often benign and asymptomatic, can pose significant risks when they compromise the visual axis or induce secondary complications. A tailored management approach is essential, beginning with observation for non-threatening lesions and escalating to aspiration, adjunctive sclerotherapy, laser treatment, or surgical excision when necessary (Table 2). Accurate differentiation from iris melanoma remains paramount, given the vastly different prognoses and therapeutic pathways. Advances in imaging and minimally invasive techniques continue to improve diagnostic precision and therapeutic outcomes, particularly in pediatric and visually vulnerable populations.
