ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Division of Endocrinology, Pedro de Elizalde Children’s General Hospital, Buenos Aires, Argentina.
2Interamerican Open University-CONICET, Center for Advanced Studies in Human and Health Sciences, Montes de Oca Avenue 745, 2nd Floor - (Postal Code 1270AAH), Buenos Aires.
Interamerican Open University-CONICET, Center for Advanced Studies in Human and Health Sciences, Montes de Oca Avenue 745, 2nd Floor - (Postal Code 1270AAH), Buenos Aires.
Tel: 18560086561;
Email: caoyuanecho@163.com
Received : May 08, 2025,
Accepted : Jun 23, 2025
Published : Jun 30, 2025,
Archived : www.jclinmedcasereports.com
Keywords: Left coronary artery aneurysm; Thrombosis; Multimodal imaging examination.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cao Y (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
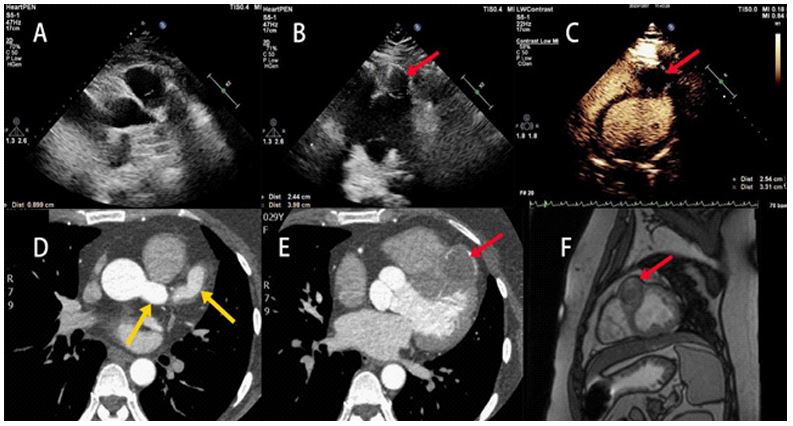
A 29-year-old woman presented with persistent chest pain for 2 days. Echocardiography revealed a dilated vessel on the left side of the aortic root (9 mm diameter; Figure 1A), and a localized hypoechoic bulge in the mid-anterior interventricular septum (24 mm × 40 mm; Figure 1B, red arrow). Myocardial Contrast Echocardiography (MCE) was performed using sulphur hexafluoride microbubbles. A well-defined hypoechoic area was observed anterior to the interventricular groove with the size of 25 mm × 33 mm. After high-energy microbubble destruction (flash imaging), the region showed no contrast enhancement (Figure 1C, red arrow). To further clarify the coronary artery condition, coronary CTA was performed. Coronary CTA demonstrated dilation of the left main coronary artery (15.6 mm) and proximal left anterior descending artery (14.5 mm) (Figure 1D, yellow arrows). The mid-segment formed a 32 × 31 mm aneurysm containing an intraluminal thrombus (Figure 1E, red arrow). To confirm the nature of the mass, a Cardiac Magnetic Resonance Imaging (CMR) examination was performed. CMR revealed an irregular tubular structure in the anterior interventricular sulcus with heterogeneous T2 signal intensity. Delayed enhancement sequences showed no significant enhancement, consistent with chronic thrombosis. The maximum cross-sectional area was about 3.6 cm × 2.8 cm (Figure 1F, red arrow). Multimodal imaging confirmed a left coronary artery aneurysm with thrombosis. Although childhood Kawasaki disease is the most common etiology of coronary artery aneurysms, the patient showed clinical improvement with anticoagulation and was discharged on rivaroxaban therapy.