ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Radiology, Children’s Hospital, Rabat, Morocco.
2Assistant Professor of Radiology, Children’s Hospital, Rabat, Morocco.
3Professor of Radiology, Children’s Hospital, Rabat, Morocco.
Department of Radiology, Children’s Hospital, Rabat, Morocco.
Email: drgabrielcao@hotmail.com
Received : Jun 26, 2025,
Accepted : Jul 14, 2025
Published : Jul 21, 2025,
Archived : www.jclinmedcasereports.com
Small arachnoid membrane protrusions into the dural venous sinuses that aid in the drainage of cerebrospinal fluid are known as Arachnoid Granulations (AGs). AGs are typically asymptomatic and only a few millimeters in size, but they can sometimes grow into Giant Arachnoid Granulations (GAGs). Rarely, GAGs can spread into the scalp or into the spaces of the bone marrow. Here, we report the accidental discovery of a GAG in a five-year-old child’s sigmoid sinus. This case emphasizes how crucial it is to identify this benign anatomical variation, especially in children, to avoid confusion dural venous sinus thrombosis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © EI Kadiri S (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
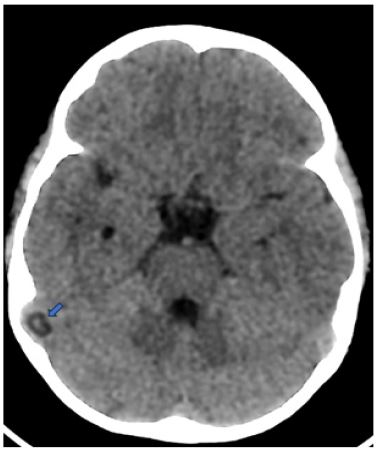
We report the case of a 5-year-old child who presented to the emergency room with febrile behavioral disturbances, including sudden-onset seizures, and visual hallucinations. Brain CT revealed a well-defined, round lesion of cerebrospinal fluid density protruding into the lumen of the right sigmoid sinus, causing a nodular filling defect. Based on its characteristic location and imaging features, the lesion was diagnosed as a giant Pacchionian granulation (Figure 1).
Arachnoid granulations can occasionally grow significantly and become Giant Arachnoid Granulations (GAGs), which can exhibit nodular filling deficiencies on venography and be misinterpreted as pathogenic entities. GAGs can cause venous stenosis, sinus enlargement, or altered venous flow, depending on their size and position. These conditions might cause symptoms like headache, lightheadedness, tinnitus, visual abnormalities, or intracranial hypertension.
The transverse and superior sagittal sinuses, frequently close to the entrance of a superficial cortical vein, are where GAGs most frequently occur. They show up on CT as well-defined, ovoid or spherical objects of CSF density that protrude into the dural sinus or calvaria and create a focal filling deficit. Their smooth edges, customary location, and absence of edema or parenchymal involvement typically allow distinction, despite the possibility that they resemble dural venous sinus thrombosis.
Since GAGs have CSF-like signal intensity on all sequences and do not intensify upon contrast delivery, MRI aids in diagnosis confirmation. Epidermoid cysts and other differential diagnoses can be ruled out using diffusion-weighted imaging.
Other possible diagnoses include extradural masses, which must be considered when bone erosion is evident. Intradiploic epidermoid cysts are a rare possibility. Some GAGs may affect venous drainage and cause intracranial hypertension despite being frequently accidental and asymptomatic. Understanding their imaging properties is crucial to preventing incorrect diagnoses and unnecessary medical interventions.
