ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Clínica Quirúrgica B, Hospital de Clínicas, Montevideo, Uruguay.
2Department of Surgery, Sanatorio Médico Integral, Montevideo, Uruguay.
3Laboratorio Diagnósticos, Montevideo, Uruguay.
Clínica Quirúrgica B, Hospital de Clínicas, Montevideo, Uruguay.
Email: moreyyy@hotmail.com
Received : Aug 28, 2025,
Accepted : Sep 11, 2025
Published : Sep 18, 2025,
Archived : www.jclinmedcasereports.com
Caroli’s disease, type V according to Todani’s classification, is a rare condition characterized by non-obstructive cystic dilatation of the intrahepatic bile ducts. We present a successfully managed surgical case treated with II-III bisegmentectomy.
This is the case of a 48-year-old male with a history of lithiasic pancreatitis and prior cholecystectomy was admitted for recurrent abdominal pain attributed to a new episode of pancreatitis. Imaging studies revealed segmental dilatation of the left hepatic duct with filling defects consistent with intrahepatic lithiasis. II-III bisegmentectomy was performed, and the patient was discharged on the 5th postoperative day.
In conclusion, Caroli’s disease represents a diagnostic challenge due to its exceptionally low incidence. A high index of suspicion is required in patients with recurrent biliar pathology. Our case demonstrates how early surgical management through hepatectomy can provide a definitive solution with low morbidity and rapid functional recovery.
Keywords: Caroli’s disease; Hepatectomy; Hepatolithiasis; Pancreatitis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Moreira E (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Type V lesions according to Todani’s classification, commonly known as Caroli’s disease, are characterized by non-obstructive dilatation of the intrahepatic bile ducts [1,2]. The most widely accepted etiopathogenic theory links this condition to a congenital malformation of the intrahepatic bile ducts, which predisposes to recurrent inflammatory episodes. Over time, these episodes lead to localized ductal destruction with subsequent dilatation. With a lower prevalence than Caroli syndrome, its incidence is 1 per 1,000,000 population [3].
The clinical presentation varies, though it typically manifests as cholangitis episodes with the classic triad of pain, jaundice, and fever, potentially accompanied by asthenia and weight loss. Less frequently, it may present as acute pancreatitis [3-5].
Diagnosis is confirmed by Magnetic Resonance CholangioPancreatography (MRCP), which visualizes the biliary tree and demonstrates continuity between cystic lesions and bile ducts [6].
This condition carries an increased risk of cholangiocarcino ma development (up to 7%), necessitating strict follow-up. This elevated risk stems from chronic inflammation secondary to recurrent cholangitis and biliary stasis, both of which promote dysplasia and eventual carcinogenesis [3,6].
The objective of this study is to present a case of Caroli’s disease and describe its clinical management.
A 48-year-old man with a history of mild gallstone pancreatitis one year prior to presentation, which resolved with favorable clinical outcomes, underwent uncomplicated laparoscopic cholecystectomy before discharge.
Current illness
The patient initially presented to the emergency department with diffuse abdominal pain, for which he received symptomatic treatment and was discharged. He subsequently returned for reevaluation due to persistent pain accompanied by nausea (without vomiting), with no accompanying signs of infection, jaundice, or bowel alterations symptoms.
Physical examination
The patient appeared in good general condition, without clincal anemia, adequate hydration, normal skin perfusion, and was afebrile. Abdominal examination revealed tenderness on deep palpation in the upper quadrants and central region, with guarding but no rigidity. No palpable masses or organomegaly were detected.
Paraclinical studies
Key laboratory results are summarized in (Table 1).
| Parameter | Value | Reference range |
|---|---|---|
| Leukocytes (x10³/μL) | 11.7 | 4.8-10.8 |
| C-reactive protein (mg/L) | 8.2 | 0-5 |
| Total bilirubin (mg/dL) | 2.38 | 0.2-1.05 |
| Direct bilirubin (mg/dL) | 1.58 | 0-0.25 |
| Alkaline phosphatase (U/L) | 157 | 40-130 |
| Gamma-glutamyl transferase (U/L) | 793 | 9-40 |
| Aspartate aminotransferase (U/L) | 361 | 0-37 |
| Alanine aminotransferase (U/L) | 561 | 0-41 |
| Serum amylase(U/L) | 1291 | 28-100 |
The abdominal ultrasound demonstrated normal echogenicity of the pancreatic head and proximal body, with peripancreatic fat stranding and minimal free fluid. The remaining pancreatic parenchyma could not be adequately evaluated due to overlying bowel gas. The liver appeared normal in size and morphology without focal lesions or echotexture abnormalities. The intrahepatic bile ducts were not dilated, and the common bile duct measured 8 mm at the hilum. No gallbladder was visualized, consistent with the patient’s history of cholecystectomy. Moderate free fluid was present in the pouch of Douglas and interloop spaces, with greater accumulation on the left side.
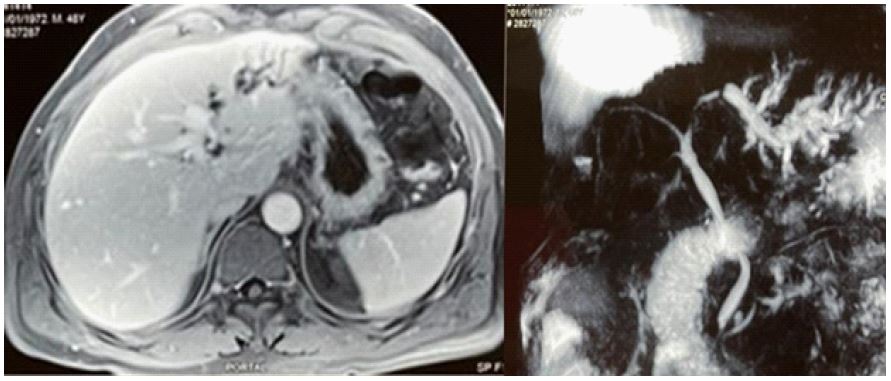
Subsequent abdominal MRI with MRCP, obtained for evaluation of suspected acute gallstone pancreatitis, revealed dilatation of the left hepatic lobe biliary system. A 9 mm filling defect with associated ductal narrowing was identified in the proximal left hepatic duct near the confluence, highly suggestive of an impacted calculus. The upstream left hepatic duct was dilated to 8 mm. Additional segmental filling defects were noted in the segment III duct along with peripheral biliary sludge deposits. The remainder of the biliary tree and hepatic parenchyma was normal, with a normal 8 mm common bile duct demonstrating appropriate distal tapering and no evidence of filling defects (Figure 1).
Clinical course
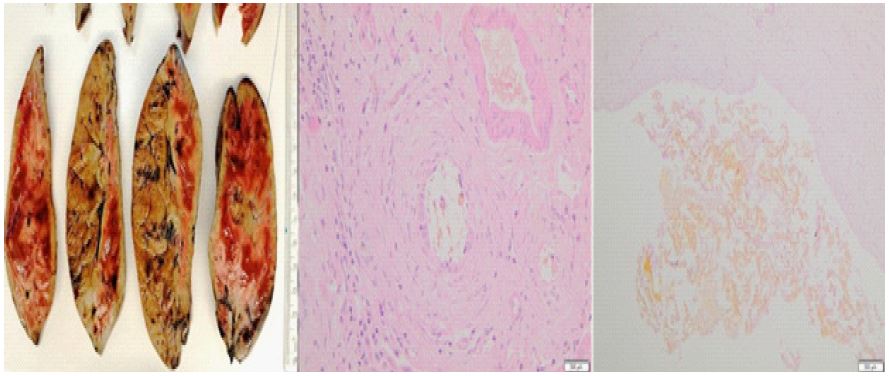
The patient demonstrated favorable recovery from acute pancreatitis and was discharged with plans for elective hepatic surgery after a 2-month interval. This delayed approach was intentionally selected to avoid performing major hepatobiliary surgery during the acute phase of pancreatitis. The procedure was subsequently performed without complications, consisting of an uneventful II-III bisegmentectomy (Figure 2).
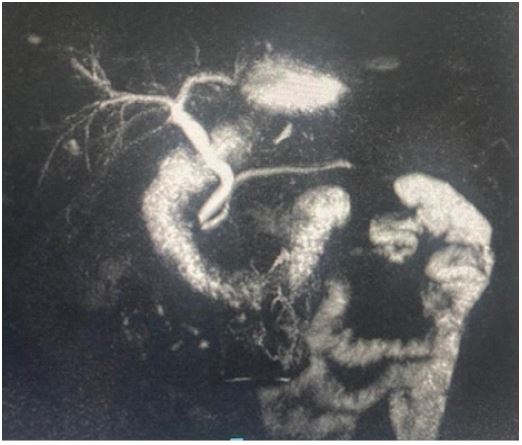
Postoperative management included 24-hour monitoring in an intermediate care unit for close observation. The patient was discharged on postoperative day 5 with an uncomplicated recovery. Follow-up evaluations in the outpatient clinic revealed complete resolution of symptoms and normalization of liver function tests. Surveillance MRCP demonstrated no residual biliary dilatation or strictures (Figure 3), confirming successful anatomical and functional resolution.
Pathology findings
The findings are consistent with hepatolithiasis, with morphological features compatible with Caroli’s disease. Associated portal hepatitis with lobular extension is evident (Figure 4).

This case emphasizes the relevance of early diagnosis of Caroli’s disease in the context of recurrent pancreatitis episodes, which enables the implementation of timely etiological treatment.
Primary intrahepatic lithiasis occurs more frequently in the left hepatic lobe due to the acute angle between the insertion of the left hepatic duct and the common hepatic duct, favoring biliary stasis [7]. In addition to anatomical factors, other causes of biliary stasis must be considered, including biliary strictures, sclerosing cholangitis, and Caroli’s disease. The latter, as hepatolithiasis, predominantly affects the left liver and is typically unilobar, as seen in our patient [3,7,8].
The late onset of symptoms in our case, whose first manifestation was gallstone pancreatitis at 47 years of age, is particularly noteworthy given that up to 80% of patients present with suggestive symptoms before 30 years of age [9]. While some authors report higher incidence in males [8], others suggest equal distribution between sexes [4].
We highlight the early resolution (15 months from the first pancreatitis episode), a situation that contrasts with the prolonged evolution described in some patients, where up to 60 months may elapse between diagnosis and definitive surgery. These delays increase the risk of cholangiocarcinoma in the resected specimen [4].
Treatment for patients with cholangitis episodes involves symptomatic management with antibiotics, abscess drainage (when present), and ursodeoxycholic acid for biliary stasis. In asymptomatic patients - either following treatment of a cholangitis episode or when diagnosis was made incidentally during routine studies - and in the absence of intrahepatic lithiasis, strict follow-up monitoring may be chosen for early detection of potential cholangiocarcinoma. For patients with associated intrahepatic lithiasis, hepatic resection is the indicated option, and in cases of bilateral involvement, the recommended treatment is liver transplantation [5,6,10].
Endoscopic drainage procedures or sphincterotomy prior to surgery are not recommended due to higher infection risk [3].
Our stance is to indicate hepatic resection even in asymptomatic patients. We opt for this approach primarily to avoid waiting for new episodes of cholangitis, which could potentially be severe, before initiating treatment. Additionally, these patients tend to develop intrahepatic lithiasis over time, and no reliable method exists for their early detection. Elevated alkaline phosphatase and gamma-glutamyl transferase levels on liver function tests do not confirm the presence of lithiasis, as these elevations are nearly constant in these patients due to existing ductal dilatation and stenosis. While ultrasound may detect lithiasis in many cases, it is not always feasible to perform serial imaging studies such as CT or MRCP.
Caroli’s disease represents a diagnostic challenge due to its exceptionally low incidence. A high index of suspicion is required in patients with recurrent biliary pathology.
Treatment individualization based on disease extent and appropriate selection of candidates for hepatic resection remain fundamental pillars in managing this condition.
Our case demonstrates how early surgical management through hepatic resection can provide a definitive solution with low morbidity and rapid functional recovery.
Conflict of interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
