ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Associate Professor, Pham Ngoc Thach University of Medicine, Vietnam.
2HCMC Eye Hospital, Vietnam.
Associate Professor, Pham Ngoc Thach University of Medicine, Vietnam.
Tel: 0903635009
Email: hoanglelan_bs@yahoo.com
Received : Aug 20, 2025,
Accepted : Sep 15, 2025
Published : Sep 22, 2025,
Archived : www.jclinmedcasereports.com
Objective: To evaluate the adjunctive treatment efficacy of Piracetam in a case of Ethambutol-Induced Optic Neuropathy (EON).
Methods: Off-label treatment trial of a clinical case report of a 38-year-old female patient presenting with rapidly progressive bilateral vision loss in 4 consecutive months after 5 months of Ethambutol therapy treating spinal tuberculosis. Past medical history included myopia. Initial Visual Acuity (VA) was Counting Fingers (CF) at 2 meters on the right eye (OD) and CF at 3 meters on the left eye (OS); pinhole vision was 20/200 in both eyes (OU); no improvement with refraction. Anterior segment examination was normal; fundus showed no optic disc damage. OCT of the optic nerve revealed thinning of the ganglion cell layer. Systemic examination, liver and renal function tests were normal. Treatment protocol: intravenous Piracetam 12 g per day for up to three treatment cycles, each lasting 10 consecutive days with a 10-day break between cycles. Treatment was discontinued once optimal visual acuity was achieved.
Results: The patient received two treatment cycles with intravenous Piracetam 12 g per day. After the first 10-day cycle, visual acuity improved to 20/50 OU. After the second 5-day cycle, visual acuity was 20/25. After 10 days post-treatment, visual acuity reached 20/20, with complete resolution of myopia. OCT of the optic nerve 1 month following revealed normalization of the ganglion cell layer. No adverse effects of Piracetam were observed. At 3-month follow-up, visual acuity remained 20/20.
Conclusion:Ethambutol-induced optic neuropathy is a notable adverse effect during tuberculosis treatment. The main treatment is to discontinue ethambutol, as vision may either partially recover spontaneously or worsen. Currently, no specific treatment exists. Common supportive therapies include B-complex vitamins supplements, especially B1 and B12. However, this off-label trial of adjunctive treatment with Piracetam suggests that Piracetam may significantly accelerate and enhance visual recovery in such cases.
Keywords: Toxic optic neuropathy; Ethambutol; Piracetam.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Le LDT (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Tuberculosis caused by Mycobacterium species is one of the most common systemic infections worldwide. Currently, Ethambutol is considered one of the main first-line anti-tuberculosis drugs in standard treatment regimens. However, it may cause adverse effects involving the liver, vision, and allergic reactions. Among these, Ethambutol-induced optic neuropathy is a notable side effect, with an incidence ranging from 1% to 6% [1], depending on the dose and duration of treatment. The onset of symptoms varies from several days to up to two years, most frequently between 4 and 12 months after initiation of Ethambutol therapy [2]. The disease is characterized by progressive, painless, usually bilateral and symmetric visual loss, rarely leading to complete blindness. Color vision disturbance is often the earliest sign, disproportionate to the degree of vision loss. In the early stage, fundus examination may be normal; in some cases, optic disc edema or pallor may be present. In the late stage, optic disc atrophy is observed, typically with temporal pallor due to loss of the papillomacular bundle fibers.
At present, there is no specific treatment for this condition; the mainstay of management remains early discontinuation of Ethambutol. Approximately 30-64% of cases show gradual visual recovery within 4-12 months after drug withdrawal, but complete recovery is rare; in some cases, visual acuity may continue to deteriorate even after discontinuation. In addition, many authors have tried various medications, with high-dose vitamin B complex- mainly vitamins B1 and B12-being the most commonly used.
Piracetam has been shown to be effective in counteracting oxidative stress in neurological conditions such as stroke and sudden sensorineural hearing loss. Moreover, previous studies have demonstrated multiple factors involved in the pathogenesis of retinitis pigmentosa, including oxidative stress. Therefore, to achieve earlier visual improvement, especially in patients whose visual acuity continues to decline markedly after discontinuing the drug, we conducted an off-label trial using Piracetam for the treatment of Ethambutol-induced optic neuropathy.
A 38-year-old female patient, Huynh Hong N., residing in Binh Chanh District, Ho Chi Minh City, presented with blurred vision in both eyes.
Medical history
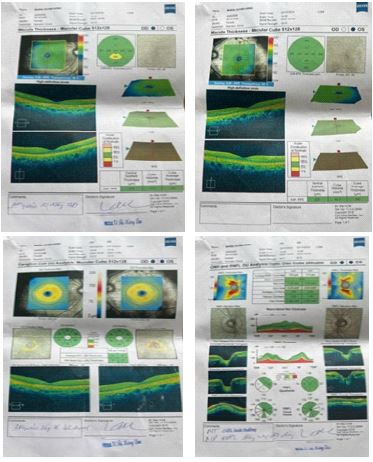
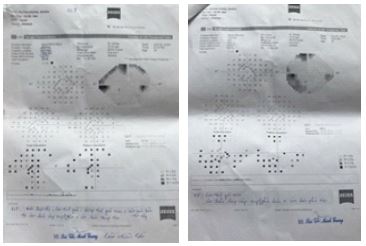
The patient reported being treated for spinal tuberculosis with an anti-tuberculosis regimen containing Ethambutol. After 5 months of treatment, she developed progressive blurring in both eyes, without pain or redness. At Ho Chi Minh City Eye Hospital, her Best-Corrected Visual Acuity (BCVA) after refraction was counting fingers at 3 meters in the right eye (OD) and 20/100 in the left eye (OS). Visual field testing showed poor fixation in OD, with suspected superior arcuate scotoma and central scotoma; OS showed an inferior arcuate scotoma and superior scotoma. OCT revealed thinning of the ganglion cell layer and macular thickness, with normal RNFL thickness in OS and mildly increased RNFL thickness in OD.
The patient was diagnosed with bilateral Ethambutol-induced optic neuropathy, and treatment included discontinuation of anti-tuberculosis drugs along with supportive therapy using Ginkgo biloba and artificial tears. After one month of drug cessation, her vision continued to decline. She visited Thanh Quan General Clinic in the fourth month of visual loss and was again diagnosed with bilateral optic nerve damage due to anti-tuberculosis medication.
OCT resulted: Both eyes: thinning of the ganglion cell layer and macular thickness. OD: mild RNFL thickening; OS: RNFL within normal limits.
Visual field resulted: OD: poor fixation, high false-negative and false-positive rates, suspected superior arcuate scotoma, and central scotoma. OS: high false-negative rate, inferior arcuate scotoma, and superior scotoma.
Past medical history
Spinal tuberculosis under treatment with a 6-month anti-tuberculosis regimen. No relevant family history identified.
Examination
• Visual acuity: OD CF at 2 meters → Pinhole: 20/200 OS CF at 3 meters → Pinhole: 20/200.
No improvement with refraction.
• Intraocular pressure: 20.6 mmHg in both eyes.
• Color vision: no dyschromatopsia detected.
• Slit-lamp examination: anterior segment of both eyes unremarkable.
• Fundus examination using Volkman Digital lens: no optic disc or macular abnormalities detected.
Additional tests before treatment
No OCT, visual field, color vision, or fluorescein angiography was performed before treatment initiation. Blood tests revealed normal liver and kidney function.
Treatment
The patient was informed that there is currently no specific treatment for this condition, and the main approach is early discontinuation of Ethambutol and waiting for possible spontaneous recovery of vision over 4-12 months. Supportive medications such as high-dose vitamin B1 and B12 have been used both in Vietnam and worldwide. However, as her visual acuity continued to worsen one month after stopping anti-tuberculosis drugs, the patient expressed a desire for earlier vision improvement. We explained the potential supportive effect of Piracetam in several neurological, ENT, and ophthalmological conditions, such as ischemic stroke, sudden hearing loss, and optic nerve ischemia, with reported positive outcomes. Additionally, we had previously treated several retinitis pigmentosa cases with Piracetam, achieving partial vision improvement [3]. Therefore, we proposed an off-label Piracetam treatment trial for the patient, which she agreed to.
Treatment protocol: Before each infusion, intraocular pressure and blood pressure were measured to ensure optimal systemic circulation of Piracetam. Intravenous Piracetam was administered slowly at a dose of 12 g per vial (based on the therapeutic dose for neurological and ENT diseases), once daily for 5-10 consecutive days per cycle. Treatment was discontinued when no further visual improvement was observed. Up to 3 cycles could be given, with a 10-day interval between cycles. After each treatment cycle, visual acuity was reassessed to determine whether to continue therapy.
Cycle 1 (November 6-15, 2024): The patient received intravenous Piracetam 12 g/vial, one vial per day for 10 consecutive days. Visual acuity improved to 20/67 in the right eye (OD) and 20/50 in the left eye (OS), with no improvement on pinhole testing in either eye. The patient was scheduled for follow-up after 10 days.
Cycle 2 (December 2-6, 2024): The patient again received intravenous Piracetam 12 g/vial, one vial per day for 5 consecutive days. On December 2, 2024, visual acuity was 20/50 in both eyes. After 5 days, visual acuity improved to 20/25 in OD and 20/29 in OS. The patient was scheduled for follow-up after 1 month.
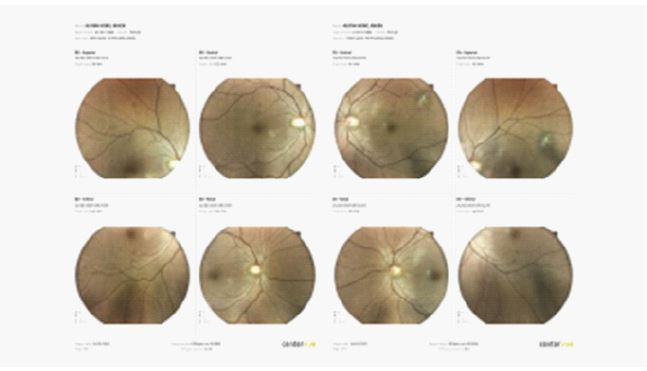
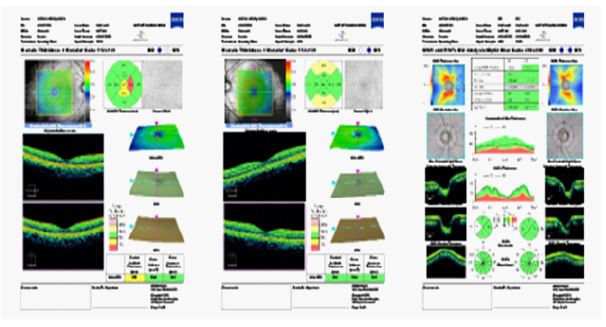
At the most recent follow-up (February 24, 2025)- two months after discontinuing treatment - visual acuity was 20/20 in both eyes, with normal color vision. No myopia was present in either eye. Fundus photography and OCT were performed. OCT of both eyes showed RNFL within normal limits and no macular abnormalities. Fundus photography revealed: OD: optic disc and macula normal; presence of peripheral choroidal scars along retinal blood vessels, most likely old tuberculosis lesions. OS: optic disc, macula, and retina are normal.
The patient was scheduled for another follow-up after 3 months. She later reported during a local follow-up visit that her visual acuity remained 20/20 with no recurrence of myopia.
Throughout the treatment period, no adverse effects of Piracetam - such as drug allergy, weight gain, hyperactivity, palpitations, asthenia, or depression - were observed. Blood tests and liver and kidney function tests remained within normal limits.
To date, tuberculosis caused by Mycobacterium species can affect multiple organs in the body, most commonly the lungs. Ethambutol, a key component of standard anti-tuberculosis regimens, can cause adverse effects involving the liver, vision, and allergic reactions. Among these, Ethambutol-induced Optic Neuropathy (EON) is a notable complication, with a reported incidence ranging from 1% to 6% [1], depending on the dose and duration of therapy.
EON typically develops within 4-12 months after starting treatment [2]. The condition is characterized by progressive, painless, usually bilateral and symmetric vision loss, rarely resulting in complete blindness. Color vision disturbance is often the earliest sign, disproportionate to the degree of vision loss. EON is classified into two types, including (1) axial/central type, with main features including decreased visual acuity, central scotoma, and red–green dyschromatopsia; and (2) peripheral type, characterized mainly by peripheral visual field loss. Early-stage clinical examination is often unremarkable, although some cases present with optic disc edema or pallor. In the late stages, pallor and optic atrophy appear, particularly temporally, due to the loss of papillomacular bundle fibers, which indicate a poor prognosis. Ancillary tests include visual field testing, color vision testing, Optical Coherence Tomography (OCT), and Visual Evoked Potentials (VEP). Visual field testing often reveals central or paracentral scotomas, peripheral constriction, altitudinal defects, and bitemporal hemianopia if the chiasm is involved. Early OCT findings may show increased RNFL thickness, particularly temporally, along with thinning of the Ganglion Cell Layer (GCL); the latter suggests progressive toxic damage.
Currently, there is no specific treatment for EON. Previous studies have reported that 30-64% of patients experience spontaneous visual recovery if Ethambutol is discontinued early; however, complete recovery is rare [4]. Tsai reported that 50% of cases recovered vision within 1-3 years after stopping the drug [5], but some patients continued to deteriorate. Various medications have been tried, most commonly high-dose vitamin B complex (B1 and B12). Animal studies have suggested that caffeic acid phenethyl ester may reduce oxidative stress. In China, some authors reported that combining a traditional medicine (buqihuoxue) with methylcobalamin improved visual acuity, visual fields, and RNFL thickness after stopping Ethambutol [6]. The degree of visual field recovery remains controversial. Chai and Lee reported recovery rates of visual field were 50% and 77% [7,8], respectively; whereas Woung found visual field defects persisted up to six months after drug withdrawal [9].
The exact pathogenesis of EON is not fully understood. Studies have shown that Ethambutol markedly reduces mitochondrial copper content, disrupting oxidative phosphorylation and causing mitochondrial dysfunction by interfering with iron- and copper-containing complexes in mitochondrial DNA. This leads to the formation of Reactive Oxygen Species (ROS), which cause tissue damage and apoptosis. Animal experiments suggest that Ethambutol selectively damages retinal ganglion cells via glutamate excitotoxicity. Other proposed mechanisms include increased mitochondrial membrane potential due to reduced cytoplasmic calcium and increased mitochondrial calcium, as well as lysosomal inhibition via zinc chelation [1].
Piracetam is a derivative of the neurotransmitter Gamma-Amino Butyric Acid (GABA) that improves neuronal metabolism by enhancing acetylcholine, noradrenaline, and dopamine activity. Studies in Alzheimer’s and Parkinson’s disease have identified oxidative stress and mitochondrial dysfunction as key contributors to neuronal death. Mitochondria are a major source of oxidative stress, and ROS overproduction can induce neuronal death via caspase-independent pathways. Piracetam has demonstrated anti-inflammatory, antioxidant, and anti-apoptotic effects, inhibiting ROS generation and improving mitochondrial function by increasing membrane fluidity [10]. Currently, Piracetam is not FDA-approved for neurological or ophthalmic diseases due to potential side effects such as hyperactivity, weight gain, palpitations, somnolence, depression, asthenia, decreased platelet aggregation, and reduced fibrinogen levels, and is contraindicated in patients with cerebral hemorrhage or renal failure [11].
In our study, adjunctive treatment of EON with Piracetam yielded a marked improvement in visual function. Globally, visual recovery rates after stopping Ethambutol are only around 50%, meaning that many patients show no improvement, and some even worsen. In our patient, visual acuity continued to decline for two months after drug cessation. At presentation, although she was still within the potential recovery window, her vision had already dropped to a level consistent with severe visual impairment (< CF at 3 meters) according to WHO criteria. Given the patient’s desire for earlier improvement, we initiated off-label Piracetam therapy. After receiving 15 vials over two treatment cycles, her vision improved substantially and recovered relatively rapidly. At two months post-treatment, her visual acuity was 20/20 in both eyes, with no residual myopia. This suggests that Piracetam may help accelerate visual recovery in EON. In addition, at the time of evaluation, the patient demonstrated no adverse effects associated with Piracetam, and both hepatic and renal function tests were within normal ranges. In terestingly, the patient had pre-existing myopia, but after treatment, she achieved unaided 20/20 vision without needing corrective lenses - a finding we cannot yet explain.
Our trial was conducted on an off-label basis, with diagnosis and follow-up relying mainly on clinical assessment. While our results provide preliminary evidence supporting Piracetam’s potential role in EON, larger studies are needed. We recommend:
• Discontinuing Ethambutol in all suspected EON cases.
• For patients with visual acuity >CF at 3 meters, monitor for spontaneous recovery with follow-up every 1-3 months. If visual acuity declines below CF at 3 meters or fails to improve, initiate intravenous Piracetam 12 g/vial.
• For patients with visual acuity
We report a case of Ethambutol-induced optic neuropathy successfully treated with adjunctive Piracetam therapy. This adverse effect is a significant concern during tuberculosis treatment, as it can lead to rapid vision loss and severely impact quality of life. Current management relies mainly on drug cessation and waiting for spontaneous recovery, sometimes supplemented with vitamins (B1, B12), but visual recovery rates remain modest (30-64%).
Our off-label trial suggests that Piracetam may significantly accelerate and enhance visual recovery, enabling patients to resume normal daily activities.
Patient consent: Consent to publish the case report was not obtained. This report does not contain any personal information that could lead to the identification of the patient.
Funding: No funding or grant support.
