ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Post-Graduate Trainee, Civil Hospital, Karachi, Pakistan.
2Thoracic Surgeon, DOW University Hospital, DUHS, Karachi, Pakistan.
3Orthopedic Surgeon, DOW University Hospital, DUHS, Karachi, Pakistan.
†These authors have been equally contributed to the article.
Post-Graduate Trainee, Civil Hospital, Karachi, Pakistan.
Tel: +92-3242940292;
Email: shaykhan30@gmail.com
Received : Aug 11, 2025,
Accepted : Sep 18, 2025
Published : Sep 25, 2025,
Archived : www.jclinmedcasereports.com
Perforation of the myocardium due to a sewing needle, although rare, is fatal; especially in children as the event poses diagnostic and treatment challenges. Therefore, we present a case of a 5-year-old female child with accidental injury caused by sewing needle that entered the myocardium.
Needle in the heart can either present symptomatically or asymptomatically and guidelines outlining the indications for extraction have yet not been established, though still under discussion, the general agreement is that removal is necessary whether the patient presents with symptoms or without. This case may offer valuable insight for future cases with similar presentations and treatment approaches.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Khan S (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Retained foreign body due to penetrating injury of the thoracic cavity is a rare medical event, responsible of approximately 1-13% of all thoracic trauma cases. Such lesions present with difficulty in treatment due to variable origins and likely cardio-vascular consequences [1]. Intracardiac lesion caused by foreign body are rare and can have perilous outcomes [2,3]. Direct penetration, intravenous migration or medical procedures are the three ways foreign objects are retained in the heart [3]. Sewing needles in the heart are usually accidental [4] and the decision between surgical and non-surgical treatment is variable according to the patient’s presentation [4,5]. As a needle in the myocardium is considered a danger to life, it can present with critical events such as cardiac tamponade, valve dysfunction, mural thrombus, embolism, and infection, particularly in pediatric patients, where it’s fatal to have a fine-point needle in the heart, and medical assessment is further challenging due to the lack of communication skills [6]. We report a case of a female child patient who underwent extraction of a sewing needle from her right ventricle.
A 5-year-old girl was referred to us, in a tertiary care hospital, from remote areas of the country. She presented with a 4-day history of mild pricking sensation in her chest. As reported by the parents, a sewing needle was placed on the child’s shirt in place of a missing button, which penetrated her anterior chest wall, while playing with other children.
As stated by the guardians, the patient was taken initially to a local hospital in their home-town, where an attempt was made to remove the foreign body; however, the procedure was unsuccessful, due to limited facilities in the operation room and lack of surgical expertise. The patient, thereafter, was referred to our tertiary care center.
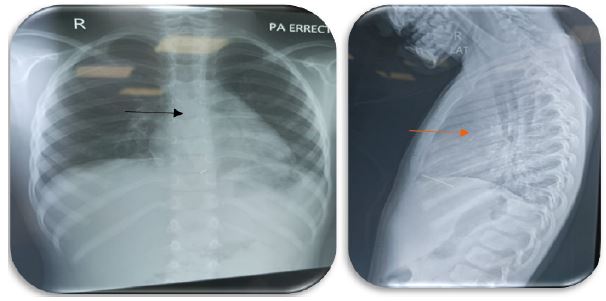
On examination, the child was alert and active, sitting comfortably with no notable signs of distress. There was a 3 x 2 cm closed wound present on the mid-anterior chest wall, with positive tenderness around the wound site, and no visible discharge. Complete cardio-vascular and chest examinations presented no abnormalities with normal breath and heart sounds. The patient had non-significant findings related to other organ systems, with no prior history of any birth-related or congenital diseases. Chest x-rays, AP and Lateral views, carried out previously in their home town demonstrated a slender radio-opaque object, present behind the lower sternum, which corelated with the mother’s report of an accidental injury with a sewing needle.
The patient was initially seen in the out-patient department of pediatric surgery. Orthopedic surgical team was taken on board, due to the unavailability of fluoroscopy and radio-lucent table in the pediatric OR, and thoracic surgery was then involved.
Although asymptomatic, all teams agreed that an urgent need to remove the needle was warranted, to prevent possible fatal complications. Pre-operative preparation was completed, with all baseline investigation returning normal results, and the patient was listed for surgery.
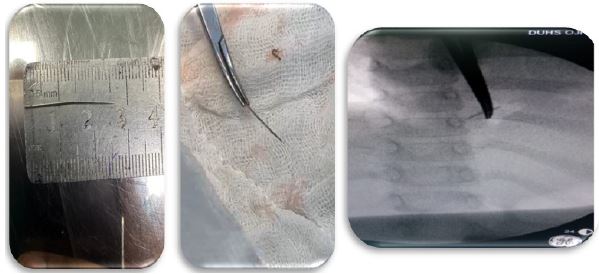
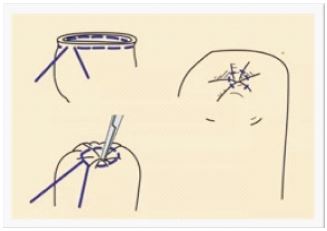
The patient was transferred to the OR, with no disturbances in vital signs. Under general anesthesia, intubation was done and monitoring lines attached. Before giving the incision, dynamic fluoroscopy was done, it was noted that the needle was rhythmically moving, raising the suspicion of it being in a vital structure. Thoracic surgeon was asked to take over, moving forward. Surgical access was gained through a sub-xiphoid incision extending cranially towards the sternum. The xiphoid itself was cut, and sternotomy was done till the body of sternum. Tissue dissection was done till the pericardium. The pericardium was opened, and 30 ml of blood was visible in the pericardial cavity. The foreign body was found penetrating the right Ventricle, with just 2-3 mm visible over the heart. Purse string sutures (Figure 3) were taken being passed through pledgets. The needle was successfully removed using a curved artery forceps, with simultaneous tying of the sutures. The pericardium was irrigated with normal saline 0.9%, a drain was placed, and closing of the structures was done layer by layer. The surgery was uneventful and successful. The patient was shifted to the pediatric intensive care unit for monitoring, with the step-down of the patient in the general ward on the second post-operative day. The drain was removed on the third post-operative day, with findings of 10-15 ml of serosanguinous fluid. She was discharged on the fourth post-operative day with no adverse outcomes.
Penetrating myocardial injury is uncommon [1-6]. Injuries such as that might be accidental in adults and children, however psychiatric conditions causing self-harm, domestic violence [4,8], acupuncture therapy and intravenous drug abuse [7,8] have been reported in literature. In such occurrences, high thoracic mobility and dynamic function increase the chances of further penetration and damage [9], progressing towards fatal outcomes which may be pericarditis, endocarditis, embolization and damage to the anatomical structures [1,4,9]. In pediatric population, low intensity symptoms and lack of proper communication skills can advertently result in delayed treatment and critical outcomes, so early assessment, timely decision-making skills and proper management can save the patient’s life [1].
In the view of the literature, echocardiography is superior to all radiological imaging modalities [3] and plays a role in giving a more accurate assessment of the silent damage carried out by the needle [1,3,6]. However, in our case due to the rare nature of the injury, immediate action was taken, to prevent critical consequences. Chest x-rays also play an important role in the early assessment and pointing towards the location of the sharp object [1]. There is debate, that although diagnostic imaging of needle-based heart lesions includes computed tomography [4,8,9], trans-thoracic [8,9] and trans-esophageal echocardiography [8] c-arm x-ray is more helpful in locating the needle and is time-efficient [4,8].
In our case, the child presented with a four-day prior history of chest-related symptoms, and due to the timely and decisive action of the teams involved, extraction of the needle from the right ventricle was successful and uneventful. Foreign bodies in the heart are rare occurrences, with sewing needle found in the myocardium, being more unlikely. Such cases should be handled with quick clinical assessment to reach an early diagnosis and with timely intervention to prevent any life-threatening complications. In our case, the child presented as a symptomatic case and conservative treatment was not advised. The patient was prepped for surgical removal, after assessing the x-rays, which were more than enough to pinpoint the needle. Further accuracy of the needle’s location was obtained through an on-table C-arm fluoroscopy. The purpose of this scenario is to highlight the urgency of the matter, which should push quick decision making, and use time efficient modalities, for a positive outcome.
Due to the uncommon nature of the medical event, there are no established guidelines for management [4,5,9]. Some authors recommend, that healed wounds without symptoms, caused by foreign bodies, warrant conservative management [5,6,8]. The decision between surgery and non-surgical management is based on patient state and risk of adversities, but the general agreement is the immediate extraction of the foreign body to prevent hazardous outcomes [1,2,4-6], especially in pediatric patients [1].
Having an accurate knowledge of thoracic anatomy is essential for a positive treatment plan to take place in piercing cardiac lesions [10]. In our case, a small access was gained with an incision on the subxiphoid level, with extension upwards till the body of sternum, for better accessibility. Upon review of the literature, different authors recommend different approaches, as no guidelines exist on the removal of a needle from the myocardium. Some authors believe that the median sternotomy should be procedure of choice [4], while some debate that initially a small access should be made, while being prepared to increase the size of the entry point [5]. In view of our case, we find that the latter provides a minimally invasive option, with extension, when poor visibility arises.
The established guidelines that can provide the accurate management of removing the needle from the heart, are not present in the literature. Regardless, acutely presenting piercing lesions in the myocardium or thorax, whether symptomatic or not, should warrant surgical removal. Our case also underscores that time efficient imaging modalities should be used to make a prompt diagnosis, to prevent possible complications. Cases like ours should be dealt in tertiary care hospitals, with available expertise, equipment and multi-disciplinary teams, that allow an efficient management plan for the patient and prevents any further harm to the patient.
Compliance with ethical guidelines: As the patient was under age, consent was gained from the parents, for all the information present in the article. Permission from the ethical was not needed, as the article is a case-report.
Acknowledgements: As this was a case study, no funding or grants were required. Professor Niaz Hussain Soomro, Professor Nusrat Rasheed, and Dr. Shayan Khan have played an equal role in writing this case report.
