ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Department of Critical Care Medicine, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, China.
Department of Critical Care Medicine, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, China.
Email: fishyyt@sina.com
Received : Aug 27, 2025,
Accepted : Sep 19, 2025
Published : Sep 26, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Yuetian Y (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
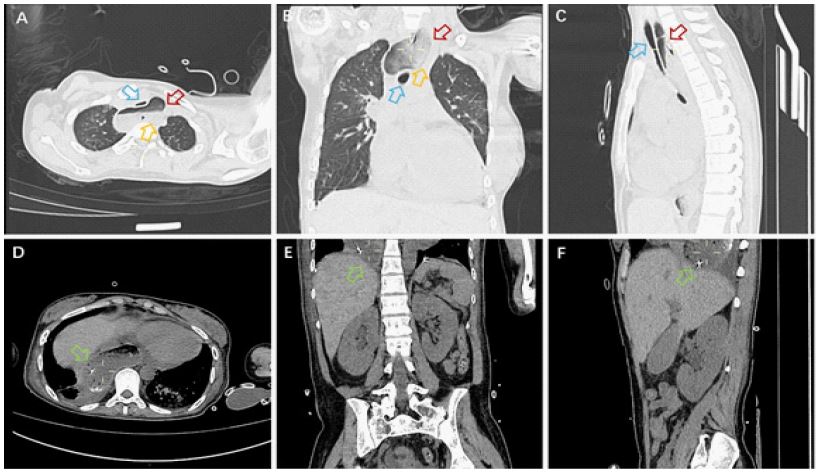
A 24-year-old female was admitted to the hospital due to muscle soreness in the limbs, retrosternal pain, and difficulty swallowing for over 50 days. Upon admission, physical examination revealed proximal muscle strength of level 3 in both upper limbs and level 5 in distal muscles, proximal muscle strength of level 4 in both lower limbs and level 5 in distal muscles, with no muscle atrophy or pseudohypertrophy observed, and normal muscle tone. Laboratory tests indicated that creatine kinase 4474 U/L, lactate dehydrogenase 330 U/L, interleukin-6 266.94 pg/ml, erythrocyte sedimentation rate 38 mm/h. The idiopathic inflammatory myopathy profile revealed a nucleolar-pattern Antinuclear Antibody (ANA) titer of 1:100 and strongly positive anti-NXP2 IgG antibodies (+++). Electromyography suggested possible myogenic damage, and chest CT indicated dilation of the upper esophagus with contents, measuring up to 5.6 centimeters at its widest point. Abdominal CT showed a gas-containing stomach sac above the diaphragm, suggesting a hiatal hernia (Figure 1). The patient was diagnosed with dermatomyositis, considering the esophageal dilation and hiatal hernia as manifestations of dermatomyositis in the digestive tract. After treatment with prednisone, methotrexate, and tocilizumab, the patient’s symptoms gradually improved.
The esophagus is a muscular tube that is divided into three sections: the cervical segment (upper segment), the thoracic segment (middle segment), and the abdominal segment (lower segment). The upper segment of the esophagus extends from the pharynx (approximately at the C6 level) to the level of the aortic arch (approximately at the T4 level) and is primarily composed of striated muscle. In a resting state, the esophagus is typically collapsed, with an internal diameter measured at approximately 1.5 to 2.5 centimeters on imaging. During swallowing, the esophagus expands, and its diameter can increase to 2 to 3 centimeters to allow food to pass through. During a barium swallow test, the maximum expansion of the esophagus can reach over 3 centimeters, but exceeding this range may indicate pathological changes, such as achalasia or scleroderma, necessitating further examination for a definitive diagnosis [1,2].
Dermatomyositis is characterized by inflammation of the striated muscles (skeletal muscles). The upper third of the esophagus consists of striated muscle, and the inflammation caused by dermatomyositis induces muscle fiber degeneration and necrosis, leading to muscle weakness and affecting the active contraction function of the upper esophagus. At the same time, the decrease in the contraction strength of striated muscles reduces the esophagus’s ability to deliver food, resulting in food retention. Prolonged retention causes passive dilation of the esophagus, particularly more pronounced in the proximal segment. Additionally, dermatomyositis may involve the autonomic nervous system, affecting the coordinated contractions of the esophageal muscles (such as decreased primary peristaltic waves), while abnormalities in nerve signal transmission lead to uncoordinated esophageal movements, further hindering the passage of food. The lower esophageal sphincter’s tension may decrease or relax abnormally, resulting in gastroesophageal reflux. Repeated reflux irritates the esophageal mucosa, causing inflammation and structural relaxation, exacerbating dilation. Dysphagia, food regurgitation, and retrosternal pain are common symptoms of esophageal dilation. Relevant examinations mainly include barium swallow studies (showing dilation and reduced peristalsis), high-resolution manometry (dynamics abnormalities), and endoscopy (to exclude other lesions). The main symptoms of dermatomyositis include low-grade fever, fatigue, photosensitivity, dyspnea, scales, papules, pruritus, pigmentation spots, depigmentation, and esophageal dilation [3,4]. If a patient shows signs of esophageal dilation and digestive endoscopy has excluded other lesions, it is necessary to differentiate these from the symptoms of dermatomyositis.
Acknowledgments: This work was supported by the Project of the Key Laboratory of Multiple Organ Failure, Ministry of Education (2023KF07, 2024KF03), the Key Laboratory of Intelligent Pharmacy and Individualized Treatment in Huzhou City (HZKF-20240101).
Contributions: (I) Conception and design: L Wang, R Li and Y Yu; (II) Administrative support: Y Yu; (III) Provision of study materials or patients: Y Yu; (IV) Collection and assembly of data: L Wang, Y Yu; (V) Data analysis and interpretation: Y Yu; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Conflicts of interest: The authors have no conflicts of interest to declare.
Informed consent: Informed consent was obtained for the use of information and images. The patient’s identity has been kept confidential.
