ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Surgery Unit, Walailak University Hospital, Walailak University, Nakhon Si Thammarat, Thailand.
Surgery Unit, Walailak University Hospital, Walailak University, Nakhon Si Thammarat, Thailand.
Email: b-bee_jung@hotmail.com, siriporn.ko@wu.ac.th
Received : Aug 26, 2025,
Accepted : Sep 19, 2025
Published : Sep 26, 2025,
Archived : www.jclinmedcasereports.com
Multiple biliary hamartomas, known as ‘Von Meyenburg Complexes’ (VMCs) are rare mostly benign bile duct malformation which are found incidentally. Most patients have no symptom, non-specific clinical presentation and absent of guidelines management are challenged. Tissue biopsy is performed to differentiate potential malignancy in suspected case. This study presented a case of a patient who had fatigue and dyspnea post covid-19 infection which incidentally found multiple liver cystic lesions, the observation and imaging follow up showed stable lesion without malignant feature.
Keywords: Biliary hamartoma; Von Meyenburg Complexes; Liver polycystic disease; Case report.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kowiwattanakarn S (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Multiple biliary hamartomas, known as ‘Von Meyenburg Complexes’ (VMCs) are rare benign bile duct malformations first described by von MeyenBurg in 1918. These are cause by the failure of embryonic remnants of bile duct involution. The prevalence estimated ranges from 0.6%-5.6% from autopsy and around 1% on imaging [1,2]. The VMCs has been reported 0.9% in children [3]. Recently they are increasing report in adults over the age of 35 [1,4]. These variety of cystic lesions of the liver are generally asymptomatic and usually incidental diagnosis on autopsy, intraoperation or imaging work up for other conditions [4,5]. Multiple liver cystic lesions must be differentiated from other lesions such as mimicking liver metastasis [6].
This article is aimed at reporting a case of VMCs present with dyspnea and incidental finding from chest Computed Tomography (CT), diagnosis, follow up and conservative treatment outcome. This case report was approved by the University Research ethics committee (WUEC-25-205-01).
A 49-year-old Thai male patient presented at OPD of School of Medicine, Walailak University Hospital, Nakorn Si Thammarat, Thailand, with fatigue and dyspnea post Covid-19 infection for 2 months. The patient denied previous medical condition or underlying disease. His vital signs were stable. On physical examination found no abnormality was detected. Initial blood work up for Complete Blood Count (CBC), renal function, liver function and thyroid function test were unremarkable (Table 1).
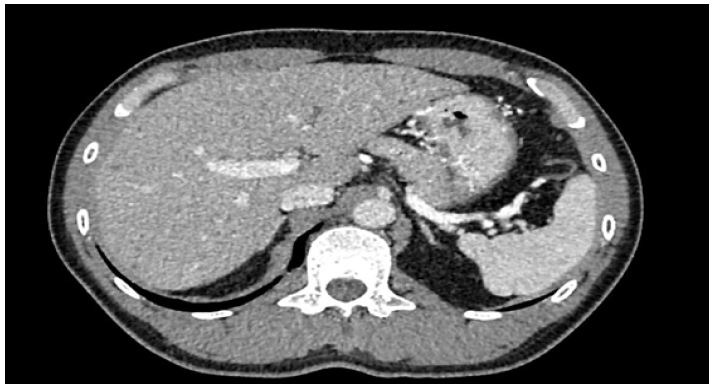
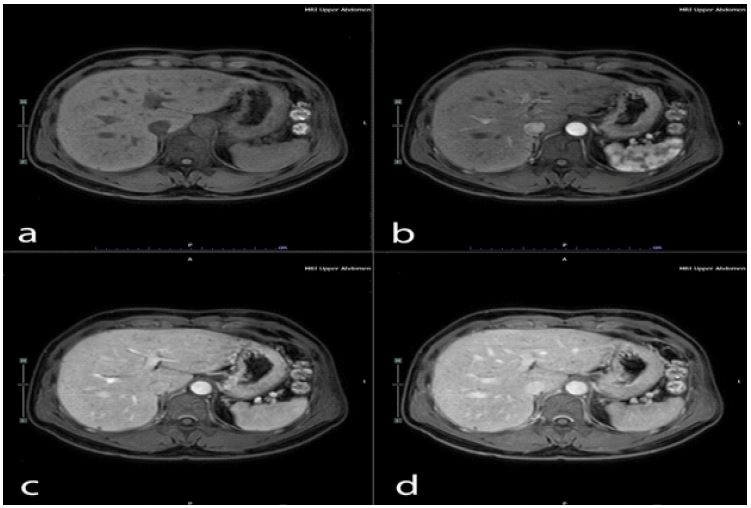
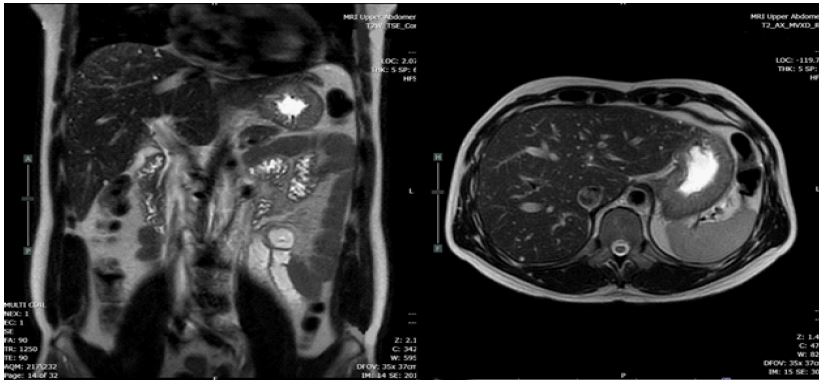
This patient was treated by medication; bronchodilator inhalator for symptomatic relief, molnupiravia (200 mg) 1 tab every 12 hours for 5 days. He was still complaining of fatigue and dyspnea. After failure of medication treatment, the electrocardiography and echocardiography were requested for re-evaluation. The result of that investigation showed normal. The CT chest was performed and reported innumerable Too Small to Characterize (TSTC) lesion scattering both hepatic lobes (Figure 1). The further Magnetic Resonance Imaging (MRI) revealed innumerable cystic lesion in both lobes of liver, (Figure 2). TW showed a signal lower than the liver parenchyma and T2W showed cystic hyperintensity like a ‘starry sky’ (Figure 3).
This patient was informed imaging result and advice observed after discussion prognosis based on current clinical evidence. Further clinical and imaging follow up 12-month to date, lesion showed stable without malignant feature on ultrasonography.
| CBC | Result value | Reference | |
|---|---|---|---|
| RBC count | 4.48 | 106 cell/mm3 | 3.75-6.54 |
| Hemoglobin | 13.7 | g/dL | 11.5-17.0 |
| Hematocrit | 40.4 | % | 37.0-54.0 |
| MCV | 90.2 | fl | 80.0-100.0 |
| MCH | 30.6 | pg | 27.0-32.0 |
| MCHC | 33.9 | g/dL | 32.0-36.0 |
| RDW | 13.2 | % | 11.0-16.0 |
| WBC count | 6490 | cell/mm3 | 4000-10000 |
| Neutrophil | 56 | % | 40-75 |
| Lymphocyte | 36 | % | 20-45 |
| Monocyte | 6 | % | 10-Feb |
| Eosinophil | 1 | % | 0-6 |
| Basophil | 1 | % | 0-1 |
| Platelet count | 253000 | cell/mm3 | 140000-400000 |
| Thyroid functiontest | Result value | Reference | |
| Free-T3 | 3.58 | pg/mL | 2.02-4.43 |
| Free-T4 | 1.31 | pg/mL | 0.93-1.71 |
| TSH | 2.76 | uIU/mL | 0.27-4.20 |
| Renal functiontest | Result value | Reference | |
| Blood Urea Nitrogen(BUN) | 12 | mg/dL | 8.4-20.6 |
| Creatinine | 0.92 | mg/dL | 0.73-1.18 |
| eGFR | 98 | mL/min/1.73m2 | |
| Liver functiontest | Result value | Reference | |
| Aspartate aminotransferase | 25 | U/L | Nov-34 |
| Alanine aminotransferase | 21 | U/L | <45 |
Multiple biliary hamartomas or ‘Von Meyenburg Complexes’ (VMCs) are a variety of benign cystic lesion of liver that consist of focal collections of duct-like structures embedded in a fibrous stroma resulting from ductal plate malformation involving the small interlobular bile ducts [7].
VMCs usually do not cause symptoms and incidental finding with recent noninvasive imaging modalities. Most of biliary hamartoma are composed of small, 5-30 mm disorganized clusters of dilated cystic bile ducts that appear throughout the liver and generally do not communicate with biliary tree [8]. The CT scan of VMCs consists of multiple small, low attenuated areas that do not enhance on contrast injection. MRI of liver and MRCP show low signal intensity on T1-weighed and high signal intensity on T2-weighed images sequences give the liver a ‘starry sky’ appearance [9-11].
Confirmation of diagnosis VMCs may require liver biopsy. In this patient, asymptomatic bilateral multiple cystic lesions and characteristic imaging finding can help avoid unnecessary invasive interventions. Most of VMCs are benign and usually conservative treatment [12].
Periodic clinical monitoring and determination of CA 19-9 can apply in asymptomatic case, but the use of CA 19-9 and other blood analysis to diagnose malignant transformation should be discouraged because it has low specificity and persistent elevation can present without malignancy [13,14]. In case of alarm symptoms or elevation of tumor marker, perform MRCP with gadolinium [15]. For suspected malignant lesion, consider tissue biopsy to confirm diagnosis. In this case, bilateral multiple cystic lesions of liver, follow up was considered after physician, patient and family discussion about prognosis. Although incidental finding and do not have symptoms, this case should be follow-up, evidence of malignant potential of VMCs has been reported [16,17].
VMCs are rare benign multiple cystic lesions of liver in adult. Treatment usually conservative and follow up. The possibility of malignancy must be discussed and considered as differential diagnosis. Periodic clinical monitor or tissue biopsy to confirm diagnosis should be applied in selected patient.
Acknowledgments: Thank to Sasima Srivisut M.D. Radiologist, Walailak university hospital for sharing MRI information in this research.
Funding: The author received no financial support for the research, authorship, and/or publication of this article.
Consent for publication: Written informed consent was obtained from the patient for his anonymized information to be published in this article.
Declaration of conflict of interest: The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure: The author of no conflicts of interest to declare.
